
Bioarchaeology International
Volume 2, Number 1: 44–62
DOI: 10.5744/bi.2018.1015
Received 10 December 2017
Revised 22 February 2018
Accepted 03 March 2018
Broken Childhoods: Rural and Urban Non-Adult Health during the Industrial Revolution in Northern England (Eighteenth–Nineteenth Centuries)
Rebecca L. Gowlanda*, Anwen Caffella,b, Sophie Newmana, Alysa Levenec and Malin Holstb,d
aDepartment of Archaeology, Durham University, South Road, Durham DH1 3LE, UK
bYork Osteoarchaeology Ltd, 75 Main St, Bishop Wilton, York YO42 1SR, UK
cOxford Brookes University, School of History, Philosophy and Culture, Faculty of Humanities and Social Sciences, Tonge Building, Oxford OX3 0BP, UK
dDepartment of Archaeology, University of York, Kings Manor and Principals House, University of York, Exhibition Square, York YO1 7EP
*Correspondence to: Rebecca Gowland, Department of Archaeology, Durham University, South Road, Durham DH1 3LE, UK
e-mail: Rebecca.gowland@dur.ac.uk
ABSTRACT During the eighteenth and nineteenth centuries, England underwent a period of rapid urbanization and industrialization. The detrimental effects of urban living conditions and child factory labor on the health of children during this time has been the subject of considerable debate and investigation by historians. It is generally understood that growing up in a rural environment was more conducive to healthy growth and development than within an industrial town. This study presents the first direct comparison of the bioarchaeological evidence for non-adult health from contemporaneous urban and rural sites from the north of England. Rural skeletal assemblages from this period are rare, and most published studies are biased toward urban sites in the south of the country. Contrary to expectations, results revealed equal prevalence rates of metabolic and dental disease at both sites, but skeletons from the rural site had greater evidence of growth disruption and respiratory disease. Evidence for specific infectious disease and medical care in response to trauma were also identified. Our interpretations of rural/urban health during this period must take into account the dire consequences of social inequalities and economic migration. There is a tendency for the latter to be characterized as unidirectional—from country to town—without due consideration of rural industry and child migrant workers.
Keywords: child labor; growth; metabolic disease
RESUMEN Durante los siglos XVIII y XIX Inglaterra experimentó un período acelerado de urbanización e industrialización. Los efectos perjudiciales de las condiciones de vida urbana y del trabajo infantil obrero en la salud de los niños durante este período han sido objeto de considerables debates e investigación por parte de los historiadores. En general, se entiende que el crecer en un ambiente rural era más propicio para un crecimiento y desarrollo saludables, en comparación con el ambiente al interior de las ciudades industrializadas. Este estudio presenta la primera comparación directa de la evidencia bioarqueológica respecto a la salud de individuos no-adultos provenientes de sitios urbanos y rurales contemporáneos del norte de Inglaterra. Las colecciones de restos óseos rurales de este período son escasas, y la mayoría de los estudios publicados están sesgados hacia los sitios urbanos del sur del país. Contrario a las expectativas, los resultados revelaron tasas de prevalencia similares en ambos sitios en cuanto a desórdenes metabólicos y enfermedades dentales, pero los esqueletos del sitio rural presentaron mayor evidencia de alteraciones del crecimiento, y enfermedades respiratorias. También se encontró evidencia de enfermedades infecciosas específicas y tratamiento médico como respuesta a traumas. Nuestras interpretaciones de la salud rural/urbana durante este período deben tener en cuenta las nefastas consecuencias de las desigualdades sociales y la migración económica. Existe una tendencia a caracterizar esta última de manera unidireccional—del campo a la ciudad—sin la debida consideración de la industria rural y de los niños trabajadores migrantes.
The eighteenth and nineteenth centuries in Britain were a period of rapid urbanization and industrialization; from A.D. 1801 to 1901 the proportion of people living in towns increased from one-fifth to four-fifths (Wohl 1983). By the mid-nineteenth century almost half of the total population of England was under 20 years of age: “England was awash with children” (Humphries 2013:115). Traditionally, children from poorer families will always have had to work, either within the domestic context or as apprentices and laborers. What changed with the Industrial Revolution was the nature of that work, with a dramatic increase in non-domestic labor by women and children (Goose and Honeyman 2013:4). Children of the urban poor in the eighteenth and nineteenth centuries have long been conceptualized as the passive, exploited victims of an insatiable industrial machine, whose wants and needs were overlooked by a laissez-faire society focussed on economy and Empire (Gowland 2015b). In a speech to the House of Lords in 1873, Lord Shaftesbury famously described children leaving the factory gates during the earlier part of the nineteenth century as “a set of sad, dejected, cadaverous creatures.… [T]he sight was most piteous, the deformities incredible. They seemed to me, such were their crooked shapes, like a mass of crooked alphabets” (Pinchbeck and Hewitt 1973:403). This account is borne out by numerous other descriptions of working-class urban children at this time (e.g., Engels 1950; Gaskell 1833). By contrast, the rural environment during this period was conceptualized as much healthier for children, offering fresh, unpolluted air, plenty of sunshine, a more varied diet, less overcrowding, and better sanitation. As Gaskell (1833:200) observed: “A child from an agricultural district, eight or nine years old, blooming with rosy health, full of vitality, is transported to a crowded town … it is exposed to miasmatic evaporations, shut up in a narrow street, its home is damp and cold, its food poor and badly cooked: in a few months, from the force of these circumstances, the Hebe-looking child has become pallid.”
These sentiments were echoed by the nineteenth-century physician Francis Sharp (in the Reports from the Commissioners on Conditions in Factories, 1833, vol XXI, parliamentary papers, pp. 12), who moved from a rural practice near Scarborough, North Yorkshire, to work in the city of Leeds: “The general appearance of the children in Leeds immediately struck me as much more pallid, and also the firmness of the fibre as much inferior to what I had seen in Scarborough and the adjacent country.… If it were not for the individuals who join the mills from the country the factory people would soon be deteriorated.”
There was a general anxiety that urban childhoods, particularly when spent undertaking factory labor, would result in the eventual physiological deterioration of the nation. These concerns sparked a number of inquiries into the health of urban and factory children, and a vast amount of qualitative and anthropometric data was commissioned from across the country. The results of these endeavors indicated that rural children were, as suspected, on average 3 cm taller than their urban counterparts (Kirby 2013). It was concluded, however, that factory labor per se was not responsible for the “stinted” growth and low life expectancy, but rather insalubrious urban conditions more generally, combined with the perceived lowly habits and morality of the poor (Chadwick 1842). There are numerous descriptions of the filthy, overcrowded, unsanitary, polluted living conditions in many of the poorer slum areas. So-called back-to-back housing in cities such as Bradford and Leeds also allowed very little natural light into the rooms, and this combined with severe air pollution meant that exposure to sunshine, vital for proper mineralization of the bones and immune function in growing children, was limited (Brimblecombe 1978; Hudson 1992). However, some contemporary accounts of rural life also point to inadequate and overcrowded houses, as well as polluted water supplies spreading diseases such as typhus (Wilkes 2011). The nineteenth-century epidemiologist William Farr felt that there was an often “fanatical” fixation on the declining conditions of urban centers, stating that “epidemics desolated the country as well as towns, though to less extent” (quoted in Young and Handcock 1956:771). Rural populations were also highly susceptible to periods of food shortages and crop failures, and a series of poor harvests could result in poverty and famine (Bogin 1999). Alfred Ireson, who was born in 1856, described rural life during this period as “a time of trial and difficulty. The agricultural workers had long hours, they pay barely enough to keep body and soul together. The condition of the children in many cases was pitiable. Rough food and clothes; everything depended on the skill and character of the mother” (quoted in Burnett 1984:83). While protective measures regarding child labor in factories were instigated, those working within agriculture and rural cottage industries were overlooked until the Education Act of 1876, which decreed that children under 10 years of age could no longer be employed in agricultural work (Burnett 1984; Pinchbeck and Hewitt 1973).
The vast majority of research concerning childhood health during this period is derived from historical data and records (Kirby 2013). While these are extremely valuable, some of the qualitative reports depict partisan viewpoints and political polemics rather than objective observation (e.g., Engels 1950). Recent excavations of cemeteries from the eighteenth and nineteenth centuries have highlighted the important contribution of bioarchaeological evidence for examining the direct physiological impact of these environments on children living at the time (e.g., Brickley and Miles 1999; DeWitte et al. 2015; Geber 2016; Lewis 2002; Mays et al. 2009; Newman and Gowland 2016; Pinhasi et al. 2006). Childhood growth and morbidity are multidimensional in etiology but are widely documented as being a sensitive indicator of the socioeconomic environment (Lewis 2007). Because so few rural sites dating to this period have been excavated, recent bioarchaeological analyses have been strongly biased toward urban population samples. Mays et al. (2008) provide a valuable comparison of urban Birmingham with rural Wharram Percy, but the latter site was in use for a millennium and predominantly medieval, thus lacking chronological resolution. This is important, because rural lifeways were not static and unchanging across the last millennium; rural industry also developed apace during the late eighteenth and early nineteenth centuries.
The aim of this study was to compare and contrast rural and urban skeletal evidence for the health and mortality of children from two sites in the north of England in order to assess the historically accepted idea that rural environments were more conducive to better childhood health. This research provides a rare insight into a rural post-medieval assemblage (now reburied) and thus also serves to enrich the existing corpus of bioarchaeological knowledge for this period, which has so far been largely confined to urban sites. This analysis of sites from the north of England also provides an important comparative data set given the current bias toward sites from the south and midlands. The bioarchaeological data will be integrated with existing historical evidence to obtain a richer understanding of living and working conditions in both environments.
Materials
Skeletal remains were analyzed from the rural churchyard of St Michael and St Lawrence, Fewston, North Yorkshire, and from the urban site of Coach Lane, North Shields, Tyneside (Fig. 1).
Fewston, North Yorkshire
Fewston is a small village located in the Washburn Valley, near Harrogate in North Yorkshire. The skeletal assemblage was excavated from the parish churchyard in advance of building work by JB Archaeology in 2009 and 2010 (Buglass 2009; Caffell and Holst 2017) and was reburied in September 2016. This assemblage is exceptional for several reasons:
1. It is one of only a few predominantly post-medieval rural skeletal collections.
2. Twenty-one of the excavated individuals were confidently identified based on coffin plates and grave monuments.
3. The diaries of John Dickinson, a late-nineteenth-century resident of the adjacent village of Greater Timble, provide important historical insights into everyday life in the Washburn Valley. The diaries also refer to a number of the identified individuals within the skeletal assemblage, thus providing unique personal insights.
The Church of St Michael and St Lawrence in Fewston was rebuilt in A.D. 1697, most of the medieval church having been destroyed in a fire the preceding year (Alred 1997:67). The graveyard would have been in use from at least the fourteenth century, and some of the excavated skeletons could date to the medieval period. Only a relatively small area (approximately 300 m2), however, was subject to excavation, and coffin plates and headstones indicated that the better-surviving burials in this location were predominantly of nineteenth-century date. The cemetery closed in 1896, although two individuals who died in the early twentieth century did gain permission to be buried there. A total of 154 individuals were excavated, including 50 non-adults, a category defined here as less than 20 years of age. The more usual cutoff age for non-adults in bioarchaeological studies is either 17 or 18 years; however, this was extended for the purposes of this study in recognition that adversity in early life (as evident in many of the skeletons within this sample) is known to cause delays in the chronological age of attainment of skeletal maturation. In the absence of a more reliable age from dental development, therefore, some of the individuals within the sample may have been slightly older than the age that their epiphyseal union suggested.
Figure 1. The location of the Fewston and Coach Lane, North Shields sites.
The use of the term non-adult in this context does not, of course, reflect nineteenth-century social norms regarding the chronological age of attainment of adult status, but denotes the skeletal age only. Parish records indicate that the social status of those buried within the cemetery was mixed, including well-off landowners as well as those of lower status, such as laborers. Agriculture was the predominant occupation in Fewston during this period, but from the late eighteenth century there was also a textile industry, with Westhouse Mill established at nearby Blubberhouses in 1791 (Alred 1997:30–31).
Coach Lane, North Shields
Coach Lane was a former Society of Friends burial ground (c. 1711–1857) located in North Shields, just east of Newcastle-upon-Tyne. North Shields in the late eighteenth and early nineteenth centuries was a heavily populated shipping, fishing, and coal-mining community, undergoing rapid development (Proctor et al. 2016). The town was heavily industrialized, and in a government report the environmental conditions were considered derisory, with narrow streets described as “more justly compared to wells filled with noxious emanations” (Second Report of the Commissioners 1845:19). Numerous epidemics, including cholera, occurred during this period, and air and water pollution from the various industries was extensive (Proctor et al. 2016). The social status of those buried at the Coach Lane cemetery was mixed, with Quakerism attracting those from different spheres of life. The burial records occasionally document the profession of the deceased, and these included “junior painter,” “grocer,” “shopkeeper,” “master mariner,” and “linen weaver.” There were many prominent, high-status Quakers within the northeast during this period, some of whom were buried at Coach Lane, along with servants (Proctor et al. 2016). The effects of a heavily polluted environment, however, would have been detrimental to all social classes (Gowland and Newman 2018). There is direct evidence that at least some of the children buried at the site had been engaged in factory labor, with the skeleton of one individual (aged 12–14 years) possibly exhibiting the notorious occupational condition “Phossy Jaw”—osteonecrosis of the mandible typically caused by exposure to phosphorus during match-making (Roberts et al. 2016). In contrast to Fewston, the Coach Lane cemetery was excavated in its entirety (Procter et al. 2016) and consisted of 236 individuals, 81 of whom were non-adults (under 20 years of age).
Methods
Age at death of the non-adults was estimated using dental development and eruption, long bone growth, and epiphyseal fusion (see Table 1 for details). Following convention, dental age was considered more representative of the chronological age of the child, as tooth development is less affected by environmental adversity than skeletal development (Elamin and Liversidge 2013; Saunders 2008—although see Discussion section below). When dental age could not be established due to missing teeth, age was instead estimated from epiphyseal fusion and metric analysis. Long bone diaphyseal lengths were measured and compared to age at death estimated from dental age as well as Maresh’s (1955) known-age long bone reference data. Skeletal growth profiles were constructed from diaphyseal lengths of the major long bones using the midpoint of the dental age range, whereby an individual with a dental age estimate falling between 0.5 to 1.5 years would be categorized as 1 year. This follows the practice of previous growth studies (see Mays et al. 2008). These age categories act as a proxy for known age, and it is not intended that the age midpoint should be taken as a genuine reflection of the precise chronological age.
Recent methods to detect growth disruption were applied, including measurements of vertebral body heights (Newman and Gowland 2015), and the left femur was selected for cortical thickness (CT) measurements (substituted with the right side when necessary) (Mays et al. 2009). Radiographs were taken using a MPX 10 portable radiography unit set at 70kVp, 0.500 mAs and with a Carestream Point-of-Care digital CR reader. Measurements of the total bone width (T) and the medullary width (M) were taken from the mid-shaft of the femur (Mays et al. 2009). Cortical thickness was determined as T – M, and plotted against the dental age (see Newman and Gowland 2016). Finally, skeletal indicators of puberty were recorded following Shapland and Lewis (2013, 2014).
The pathological lesions recorded include rickets (vitamin D deficiency), scurvy (vitamin C deficiency), cribra orbitalia, dental enamel hypoplasia, dental caries, non-specific periosteal reactions on the major long bones, endocranial and ectocranial lesions, maxillary sinusitis, rib lesions and evidence for tuberculosis (Table 1). Rickets was diagnosed through the presence of bowed long bones, flared and/or porous metaphyses and sternal rib ends, and the presence of medial tilting of the distal tibia, while coxa vara and flattening deformities in the proximal femur were also considered (Brickley and Ives 2008; Mays et al. 2006; Ortner and Mays 1998). Scurvy was diagnosed through the presence of woven bone in the orbits, porosity on the mandible and/or maxilla (especially focused on the internal ramus and coronoid process of the mandible, and around the infraorbital foramen of the maxilla), porosity on the greater wing of the sphenoid, and porosity in the supraspinous fossa of the scapula (Ortner 2003; Stark 2014). The pathological lesions associated with metabolic disease may be very subtle (Brickley and Ives 2008), and this is confounded further by the porous appearance of the rapidly growing bones of infants and children. All pathologies were therefore recorded by two bioarchaeologists working side by side (Caffell and Gowland), and the results were compared with those of an observer working independently (Newman). Rickets and scurvy were diagnosed as present only when both sets of independent observations were positive. If one independent observer identified indicators of rickets or scurvy but the other did not, then these skeletons were reexamined and agreement reached. Due to the multiple skeletal elements that can display signs of vitamin C or vitamin D deficiency, only crude prevalence rates (per individual) for these pathologies were calculated; however, individuals for whom the diagnostic skeletal elements were absent were excluded from the prevalence calculations.
Table 1. Methods of analysis used in this study.
|
Method |
References |
|||
|
Age at Death |
dental development |
|||
|
long bone growth |
||||
|
epiphyseal fusion |
Scheuer and Black 2000 |
|||
|
Growth |
cortical thickness |
Mays et al. 2009 |
||
|
vertebral body height |
Newman and Gowland 2015 |
|||
|
Pathologies |
|
metabolic disease |
|
Brickley and Ives 2006, 2008; Mays et al. 2006; Ortner 2003; Ortner and Mays 1998; Stark 2014 |
|
cribra orbitalia |
|
Stuart-Macadam 1991 |
||
|
dental enamel defects |
|
|||
|
new bone formation |
|
All long bones were examined for the presence of non-specific periosteal new bone growth in the form of woven bone, lamellar bone, and/or abnormal porosity. Likewise, the endocranial and ectocranial surfaces and maxillary sinuses were examined for new bone formation (woven and/or lamellar) and porosity. All deciduous and permanent teeth (including unerupted but observable tooth crowns) were examined for defects in enamel formation (lines, grooves or pits), and the prevalence rates for dental enamel defects were expressed as a percentage of all of the teeth present (including observable unerupted teeth). Cribra orbitalia was recorded using the Stuart-Macadam (1991) system, but only presence or absence is reported here, and results are provided as true prevalence rates (percentage of preserved orbits affected). The minimum number of ribs present on the left and right side for each individual was counted, as was the minimum number of ribs showing new bone formation (woven or lamellar). The number of un-sided rib fragments was counted, along with those exhibiting pathological lesions. Crude prevalence rates were calculated for the minimum number of ribs affected as a proportion of the minimum number of ribs present.
Results
Age at death
The age distribution of the non-adults from Coach Lane follows the pattern frequently observed at archaeological cemetery sites, with a high proportion of deaths in those under 6 years of age and relatively few deaths during adolescence (Fig. 2). By contrast, Fewston presents a more unusual non-adult age distribution, with higher numbers of adolescent deaths. Only two individuals at Fewston were less than 1 year of age, one of whom was a named individual. The lack of infants is likely to have resulted from the common practice of spatial segregation of this age group within cemeteries and the fact that only a relatively small area was excavated.
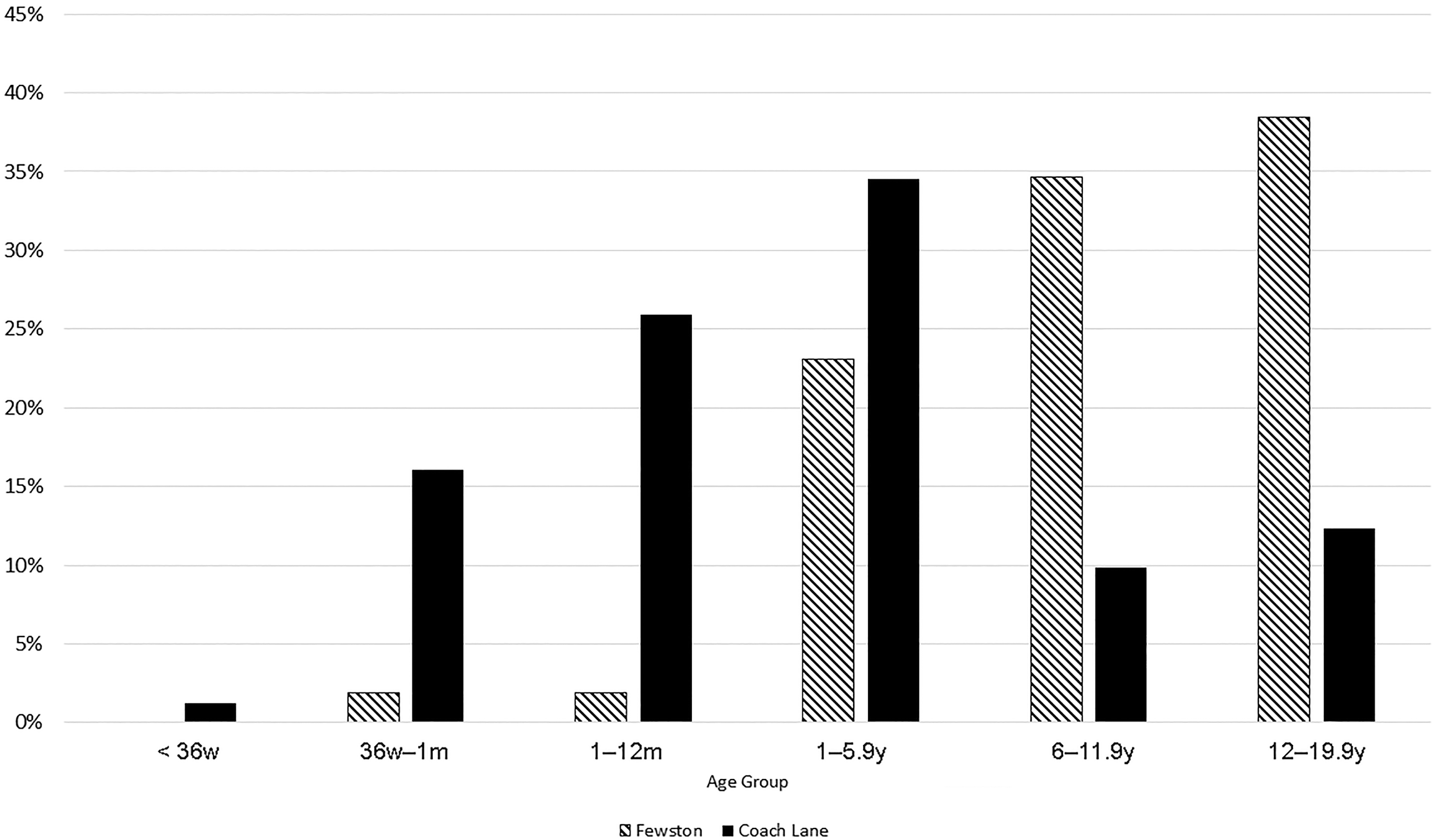
Figure 2. The age-at-death distribution of the non-adults from Fewston and Coach Lane.
The difference in age structure between the two sites with respect to the excess of adolescents at Fewston is important to consider. Is this unusual age profile simply an artifact of the incomplete excavation of Fewston, or could it reflect genuine differences in age-structure and mortality risks between the sites? If the latter, then what was the driving force behind this? We hypothesize that this difference reflects genuine mortality risks in this section of the cemetery, which is dominated by nineteenth-century burials, and that it is driven by the migration of adolescents from poor urban areas seeking employment in rural industry. This will be explored further with reference to the results for the pathological lesions below. Comparison of the various pathologies between the two sites will also explicitly consider the different age-at-death profiles when inferring aspects of the lived experiences of these children.
Growth
Diaphyseal lengths, when plotted against dental age, were similar between Fewston and Coach Lane; unfortunately, relatively few measurements were possible from the former site due to poorer preservation (Fig. 3). These values aligned with Maresh’s (1955) data up until approximately 10 years of age, after which most adolescents drop below the modern values. This could relate to the relatively delayed pubertal growth spurt in these individuals compared to modern children (Fig. 4). In keeping with the findings of Mays et al. (2009), cortical thickness appears to be a more sensitive indicator of adversity and was compromised in children from both sites. Growth retardation was observed particularly in children older than 4 years of age (Fig. 3). While only small numbers of femora were available for measurement from Fewston, cortical thickness measurements of the humeri and tibiae from these sites were similarly reduced when compared to modern norms.
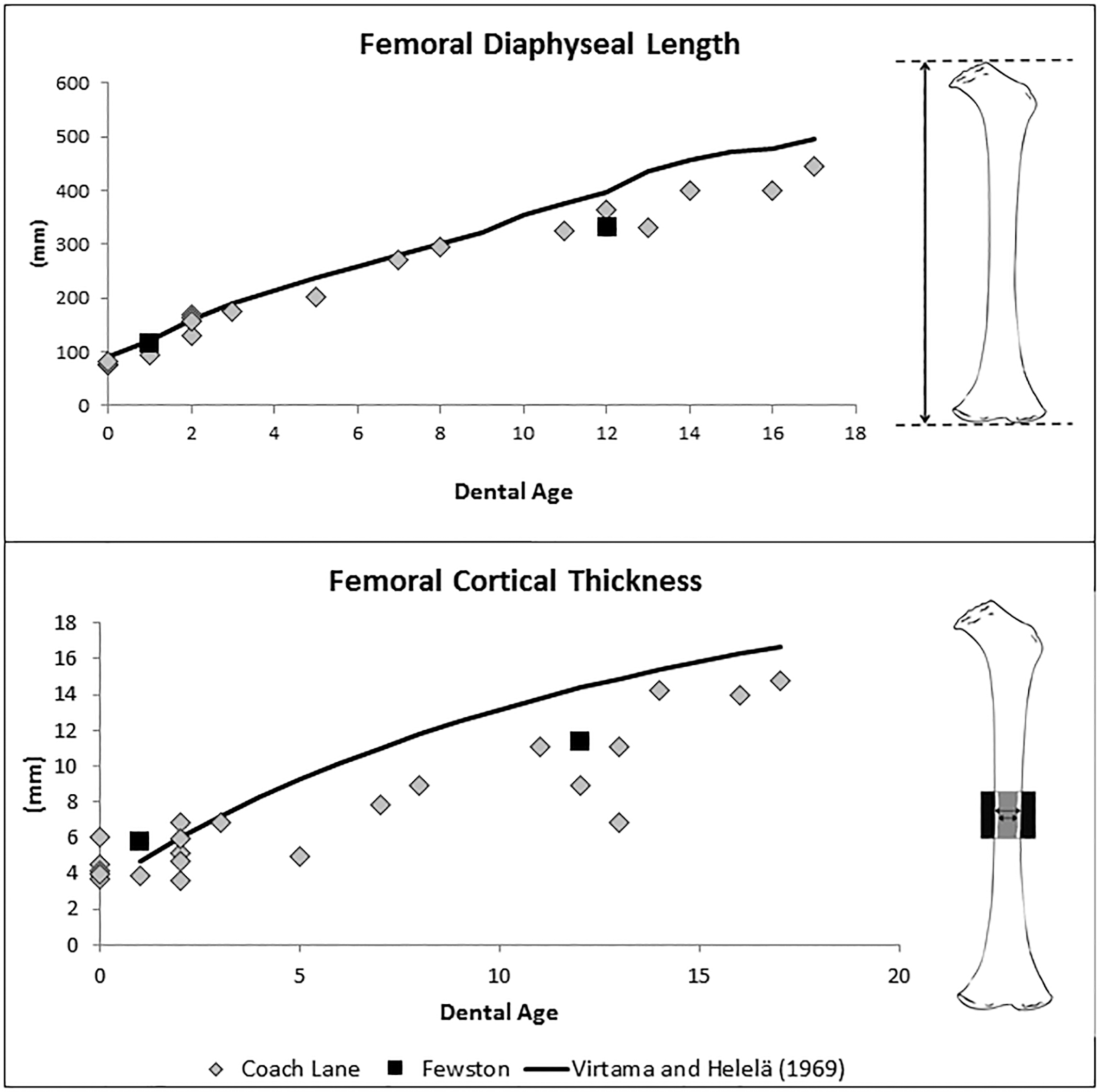
Figure 3. Femoral diaphyseal lengths and cortical thickness from Fewston and Coach Lane plotted against dental age as a proxy for known age and modern comparative data.
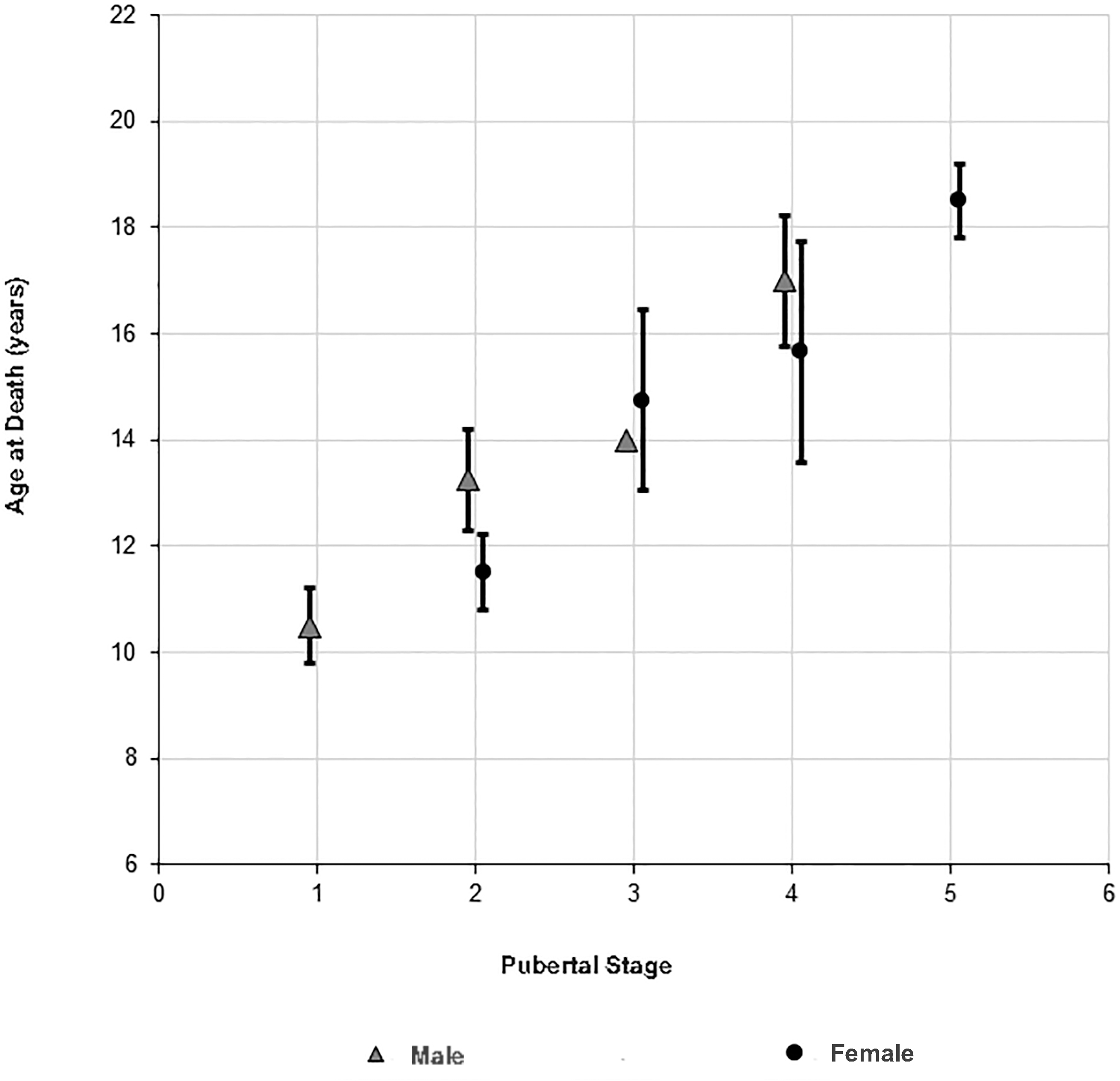
Figure 4. Pubertal stages in Coach Lane (n = 11) and Fewston (n = 24) males and females plotted against dental age.
Vertebral measurements were taken following the protocol outlined by Newman and Gowland (2015), which identified measurements from vertebral groupings of C5-6, T6-8, and L2-4 as being reliable indicators of potential population differences in growth patterns. Due to the C5–C6 group presenting a more robust sample within this study for both sites, these measurements were plotted against dental age (Fig. 5). Values for several adolescents from Fewston were anomalously low, and an ANCOVA test revealed that vertebral body height was statistically different (F[1,35] = 13.551, p = 0.001) between the two sites, while adjusting for dental age. These adolescents also exhibited a range of skeletal indicators of poor health. For example, skeleton 262 had extensive new bone formation and severe enamel hypoplasia; skeleton 338 had severe marrow hyperplasia, woven bone on multiple skeletal elements, and evidence of scurvy; skeleton 208 had sinusitis and cuspal enamel hypoplasia as defined by Ogden et al. (2007); and skeleton 331 had evidence of scurvy, rickets, enamel hypoplasia, and new bone formation on the ribs.
Pathology
A wide range of pathological lesions were observed in the non-adult skeletons from both sites. Dental enamel defects were common in both the deciduous and permanent dentitions. A greater proportion of non-adults at Fewston expressed dental defects than at Coach Lane (72% compared to 50%), but the true prevalence rate for defects was similar at both sites (Table 2), with no statistically significant difference between them (two sample t-test, p > 0.1).
There were some differences in the type of the dental enamel defects, however, with plane-form and cuspal enamel defects more frequent at Fewston (4% of all teeth compared to 0.6% at Coach Lane). Deciduous as well as permanent teeth were affected by enamel hypoplasia at both sites, including pitting defects, but cuspal enamel defects in deciduous teeth were not common (Supplementary Tables S1–S4). In such instances, the period of stress that produced these lesions would have commenced in utero and occurred during the formation of both the deciduous and permanent dentition.
The crude prevalence of rickets was similar between sites and is very high compared to contemporaneous sites in London (Lewis 2002). Likewise, the prevalence of scurvy was high, and there was no statistically significant difference between Coach Lane and Fewston (Table 3). Again, this prevalence was higher than at the London sites of Chelsea Old Church, St Benet Sherehog, and Bow Baptist (ranging from approximately 4–10%) but were more comparable with rates seen at Cross Bones (37%), a site that was located in a particularly impoverished parish of London during this period (Newman and Gowland 2016). Developments in the diagnostic criteria for both rickets and scurvy since some of these reports were published are partly responsible for the disparity, along with the exclusion of poorly preserved skeletons from the prevalence calculations in this study. The north of England, however, was a renowned focal point for rickets in the nineteenth century (Owen 1889). The prevalence rate of cribra orbitalia was, again, high at both sites, but Fewston exhibited significantly higher frequencies (Table 3).
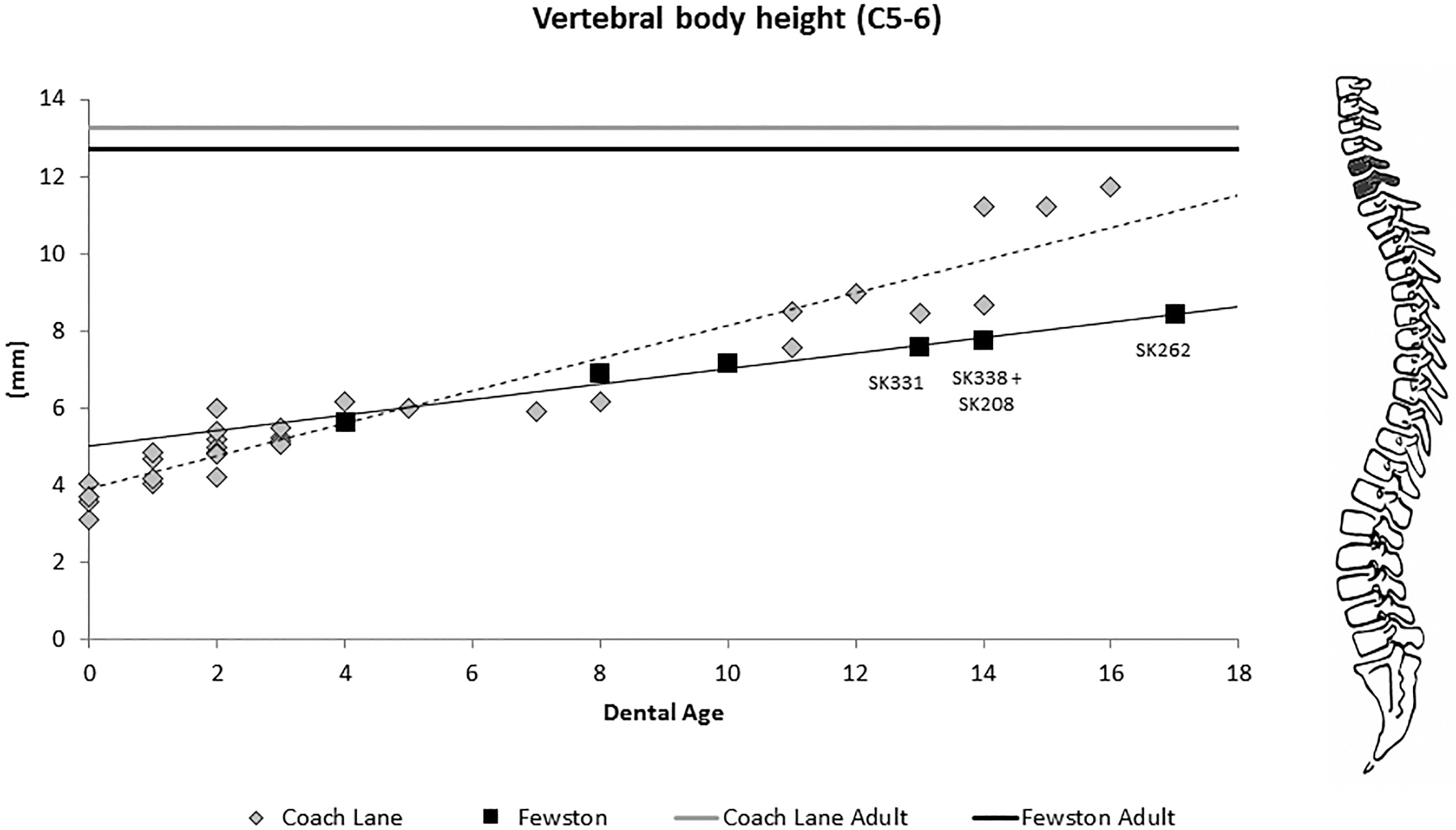
Figure 5. Vertebral body height for C5–C6 plotted against dental age.
Table 2. Dental enamel hypoplasia (DEH) at Coach Lane and Fewston.
|
Age Group |
Deciduous Teeth |
Permanent Teeth |
||||||||||||||
|
Coach Lane |
Fewston |
Coach Lane |
Fewston |
|||||||||||||
|
No. teeth (no. DEH) |
% DEH |
No. teeth (no. DEH) |
% DEH |
No. teeth (no. DEH) |
% DEH |
No. teeth (no. DEH) |
% DEH |
|||||||||
|
< 36w |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
||||||||
|
36w–1m |
34 (0) |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
||||||||
|
1–12m |
128 (13) |
10 |
7 (0) |
0 |
3 (1) |
33 |
8 (0) |
0 |
||||||||
|
1–5.9y |
382 (66) |
17 |
131 (12) |
9 |
108 (30) |
28 |
202 (28) |
14 |
||||||||
|
6–11.9y |
45 (8) |
18 |
67 (7) |
10 |
108 (37) |
34 |
338 (72) |
21 |
||||||||
|
12–19.9y |
0 |
0 |
3 (0) |
0 |
243 (114) |
47 |
475 (139) |
29 |
||||||||
|
Total |
589 (87) |
14 |
208 (19) |
9 |
462 (182) |
39 |
1023 (239) |
23 |
||||||||
Non-adults at both sites showed evidence of maxillary sinusitis and rib lesions, but the prevalence of both was significantly higher at Fewston (Table 4, rib lesions p < 0.05; sinusitis, p < 0.1) and most particularly in children of working age (12–20 years). By contrast, endocranial and ectocranial new bone was slightly higher at Coach Lane, although this was not statistically significant (Table 4). At Coach Lane, infants from 1–12 months were much more likely to exhibit endocranial new bone growth (70%) than other age groups, whereas at Fewston higher prevalence rates were observed again among the adolescents. Care must be taken when interpreting cranial lesions in such young infants, because rapid bone growth during infancy may be mistaken for pathological lesions (Lewis 2007). Periosteal new bone formation was recorded for all the major long bones and was much more prevalent among the Coach Lane population compared to Fewston. Periosteal new bone formation at this site was most frequently expressed in the tibiae (55%), while at Fewston the femur was more frequently affected (22%) (Table 5).
In terms of specific diseases among the non-adults, there were three individuals of particular note. The first was skeleton 69 from Coach Lane, who had severe osteonecrosis of the mandible accompanied by woven bone formation. This has been interpreted as likely due to phosphorous poisoning, which was a notorious occupational condition associated with the match-making industry at this time. A detailed description of this individual was provided by Roberts et al. (2016).
Table 3. Crude prevalence rates (CPR) of rickets and scurvy by age group and true prevalence rates (TPR) of cribra orbitalia (CO) at Coach Lane and Fewston.
|
Age Group |
Coach Lane |
Fewston |
Coach Lane |
Fewston |
Coach Lane |
Fewston |
||||||||||||||||||
|
Rickets |
CPR |
Rickets |
CPR |
Scurvy |
CPR |
Scurvy |
CPR |
CO |
TPR |
CO |
TPR |
|||||||||||||
|
36w–1m |
0 (9) |
0 |
0 (0) |
0 |
7 (8) |
87.5 |
1 (1) |
100 |
2 (22) |
9 |
0 (1) |
0 |
||||||||||||
|
1–12m |
7 (12) |
58.3 |
1 (1) |
100 |
10 (12) |
83.3 |
1 (1) |
100 |
2 (20) |
10 |
0 (1) |
0 |
||||||||||||
|
1–5.9y |
11 (25) |
44.0 |
2 (4) |
50 |
7 (27) |
25.9 |
3 (8) |
37.5 |
17 (51) |
37 |
3 (6) |
50 |
||||||||||||
|
6–11.9y |
3 (7) |
42.8 |
6 (9) |
66.6 |
0 (6) |
0 |
4 (13) |
30.8 |
6 (10) |
66.6 |
7 (9) |
77.8 |
||||||||||||
|
12–19.9y |
7 (10) |
70 |
4 (15) |
26.6 |
2 (10) |
20 |
6 (16) |
37.5 |
8 (19) |
50 |
9 (14) |
64.3 |
||||||||||||
|
Total |
28 (63) |
44.4 |
13 (29) |
44.8 |
26 (63) |
41.2 |
15 (39) |
38.4 |
35 (122) |
32.8 |
19 (31) |
61.3 |
||||||||||||
Table 4. Prevalence rates by age and site for maxillary sinusitis (Sinus), rib lesions (Rib), ectocranial lesions (Ecto) and endocranial lesions (Endo) at Coach Lane and Fewston. True prevalence is provided for maxillary sinusitis, while only crude prevalence rates are given for the other pathologies.
|
Age Group |
Coach Lane |
Fewston |
||||||||||||||||||||||||||||||
|
Sinus |
TPR |
Rib |
CPR |
Ecto |
CPR |
Endo |
CPR |
Sinus |
TPR |
Rib |
CPR |
Ecto |
CPR |
Endo |
CPR |
|||||||||||||||||
|
< 36w |
0 (0) |
0 |
0 (1) |
0 |
0 (1) |
0 |
0 (1) |
0 |
0 (0) |
0 |
0 (0) |
0 |
0 (0) |
0 |
0 (0) |
0 |
||||||||||||||||
|
36w–1m |
2 (2) |
100 |
1 (11) |
9.1 |
3 (13) |
23 |
4 (13) |
30.7 |
0 (0) |
0 |
0 (1) |
0 |
1 (1) |
100 |
1 (1) |
100 |
||||||||||||||||
|
1–12m |
1 (2) |
50 |
1 (19) |
5.3 |
12 (20) |
60 |
14 (20) |
70 |
0 (2) |
0 |
0 (1) |
0 |
1 (1) |
100 |
1 (1) |
100 |
||||||||||||||||
|
1–5.9y |
6 (24) |
25 |
1 (25) |
4 |
5 (28) |
17.9 |
12 (28) |
42.9 |
4 (7) |
57.1 |
0 (5) |
0 |
1 (10) |
10 |
4 (10) |
40 |
||||||||||||||||
|
6–11.9y |
0 (9) |
0 |
0 (4) |
0 |
3 (6) |
50 |
3 (6) |
50 |
4 (12) |
33.3 |
3 (12) |
25 |
0 (13) |
0 |
4 (12) |
33.3 |
||||||||||||||||
|
12–19.9y |
6 (19) |
31.6 |
4 (9) |
44.4 |
2 (10) |
20 |
2 (10) |
20 |
17 (26) |
65.4 |
5 (12) |
41 |
5 (16) |
31.3 |
5 (14) |
35.7 |
||||||||||||||||
|
Total |
15 (56) |
26.8 |
7 (69) |
10.1 |
25 (78) |
32 |
35 (78) |
44.9 |
25 (47) |
53.2 |
8 (31) |
25.8 |
8 (41) |
19.5 |
15 (38) |
39.4 |
||||||||||||||||
Table 5. True prevalence rates of periosteal new bone formation on the major long bones at Coach Lane and Fewston.
|
Age Group |
Coach Lane |
Fewston |
||||||||||||||||||||||
|
Hum |
Rad |
Ulna |
Fem |
Tib |
Fib |
Hum |
Rad |
Ulna |
Fem |
Tib |
Fib |
|||||||||||||
|
36w–1m |
10 |
21 |
38.9 |
20 |
44.4 |
12.5 |
0 |
0 |
0 |
0 |
0 |
0 |
||||||||||||
|
1–12m |
32 |
54.5 |
50 |
28 |
70.8 |
46.2 |
20 |
0 |
0 |
0 |
0 |
0 |
||||||||||||
|
1–5.9y |
16 |
2.4 |
2.6 |
38.8 |
66.7 |
21 |
22.2 |
0 |
0 |
20 |
16.7 |
33.3 |
||||||||||||
|
6–11.9y |
11 |
0 |
11.1 |
35.7 |
8.3 |
9 |
6.7 |
0 |
0 |
28.6 |
25 |
20 |
||||||||||||
|
12–19.9y |
27.7 |
22 |
27.8 |
36.8 |
50 |
22.2 |
4 |
0 |
16.6 |
20.8 |
10.3 |
15.8 |
||||||||||||
|
Total |
20 |
15 |
21 |
32.8 |
55 |
21.9 |
9.8 |
0 |
7.9 |
22 |
13.6 |
18.5 |
||||||||||||
Skeleton 223 (14–15-year-old) from Fewston had multiple lytic lesions accompanied by new bone formation in the skull. Unfortunately, the skull of this individual was highly fragmented and only parts of the skull, vertebrae, and upper ribs were preserved. Both orbital roofs had thick deposits of lamellar bone, with woven bone also present in the left orbit. A circular lytic lesion approximately 14 mm in diameter, with sharp, clear margins, had penetrated the thickness of the right orbital roof (Fig. 6). Four further lytic lesions were present elsewhere on the cranium. The surrounding external surfaces of these generally had scalloped roughened areas, with deposits of partially remodeled woven bone and lamellar bone (Fig. 7). The body of the vomer was enlarged and covered with well-remodeled lamellar bone, with a smooth circular depression in both lateral walls and the perpendicular plate was absent (apparently remodeled). A large, shallow lytic lesion was present on the internal surface of the right mandibular ramus, and the margins were again bounded by thick deposits of partially remodeled woven bone. Deposits of lamellar bone extended along the inferior surface of the right mandibular body, and a plaque of lamellar bone was present on the external surface of the right ramus. The axis had a lytic lesion on the external surface of the left lamina surrounded by partially remodeled woven bone. An upper right rib had a deposit of porous lamellar bone on the visceral surface of the neck. None of the other rib fragments had any evidence for lesions, but few of the rib heads and necks survived.

Figure 6. Lytic lesions penetrating the right orbit of skeleton 223.

Figure 7. Lytic lesion and new woven and lamellar bone on the left frontal bone of skeleton 223.
Tuberculosis manifested in the skull, while uncommon in adults, can occur more frequently in children (Dawson and Robson-Brown 2012; Ortner 2003:247–248). Multiple cranial lesions, usually circular, less than 20 mm in size, which penetrate the thickness of the vault, as observed here, are all features of childhood tuberculosis. While bone formation around the lesions is not typical, it can occur (Dawson and Robson-Brown 2012; Ortner 2003). Chaudhary et al. (2004) and Sheikh et al. (2012) state that involvement of the jaw is more likely in older individuals (but can occur in children) and typically manifests as destructive lesions in the mandible, with potential involvement of the temporo-mandibular joint. Tuberculosis of the orbit is more common in children and is typically unilateral (Dalvin and Smith 2016), as expressed here. Blindness is a frequent complication of ocular tuberculosis (Dalvin and Smith 2016; Shameem et al. 2009), and, given the severity of the lesions, it seems likely that skeleton 223 experienced a similar outcome. Endocranial new bone formation and rib lesions have also both been associated with tuberculosis (Lewis 2004, 2007; Matos and Santos 2006; Roberts and Manchester 2005:190; Santos and Roberts 2001, 2006).
Finally, the skeleton of a 12–14-year-old from Coach Lane (skeleton 157) exhibited direct evidence of medical care in the form of cranial surgery in association with trauma. The individual had suffered a perimortem blunt-force injury to the left frontal and parietal bones along the coronal suture (Fig. 8). Two fracture lines radiated anteriorly and posteriorly from the point of impact. Two concentric fracture lines extended from the anterior fracture from a point located 44 mm superior to the left orbit rim and 20 mm anterior to the coronal suture. On the ectocranial surface a smoothly curved concentric fracture line extended superiorly and posteriorly, terminating in the coronal suture 45 mm from bregma. The lateral segment was not detached, but displaced internally slightly at the inferior/medial end. At this inferior part the fracture extends at an angle through the bone to the internal surface, where a fracture line extends superiorly for 13.6 mm. A neat circular perimortem trepanation is located in the left frontal squama 11.7 mm medial to the curved fracture line, 5.2 mm from the coronal suture, and 12.8 mm from the metopic suture. The external diameter (16.7 mm) is slightly larger than the internal diameter (14.1 mm) (Fig. 8). While the external margins are slightly crushed, the internal margins are sharp and the walls are smooth. This represents an unsuccessful attempt to provide life-saving medical treatment in response to the perimortem injury.

Figure 8. Frontal and parietal bone of skeleton 157 with perimortem trauma (B), a concentric fracture (A) and evidence for surgical intervention (C).
Discussion
The results initially appeared to contradict the sentiments espoused at the time, namely, that urban environments were much more damaging to childhood health than a rural upbringing. Skeletal remains from both places show very high levels of metabolic disease and other non-specific indicators of physiological disruption. The higher prevalence of many of the pathological conditions, together with poorer growth, among some of the children from Fewston compared with Coach Lane was contrary to expectations and historical records. Two questions arise from these results: why did the children at Fewston suffer so much chronic health stress, and why were there so many adolescents at this site? Usually, the adolescent age category is one of the least well represented within archaeological cemetery populations (as observed at Coach Lane), a factor lamented in recent studies of puberty in the past (Arthur et al. 2016; Lewis 2016; Shapland and Lewis 2013).
A direct interpretation of this skeletal evidence would lead to the conclusion that the rural environment was at least as deleterious to health as the urban environment. Historical evidence for the Washburn Valley, in which Fewston is located, does in fact point to inadequate, overcrowded, and unsanitary housing for some rural dwellers, along with polluted water supplies. For example, local resident John Dickinson noted in his diary entry for 13 October 1881: “There is part [some] talk about the deficient water supply and drainage of the village, and it is thought the sanitary authority will take the matter in hand themselves and compel the proprietors to alter things. The proprietors fear the cost and so it happens that we drink water highly polluted with sewage and our sinks [drains] are simply beastly” (Caffell 20151). In 1840, Elizabeth and William Scaife lost three children (John, aged 2 years, Hannah, aged 9 years, and Christiana Eliza, aged 6 years) within just one week to typhus fever, spread via contaminated water during an epidemic that lasted from 1838 to 1840.
While such infectious diseases undoubtedly took a toll on the morbidity and mortality of the Fewston population, they would have proven more fatal to younger children, rather than adolescents, as the dreadful suffering of the Scaife family attests. These diseases are also acute; they will kill quickly and leave no visible sign on the skeleton. They are not, therefore, responsible for the evidence of chronic disease observed among many of the adolescent skeletons. When interpreting the prevalence of pathological lesions, the younger age-at-death profile of the children at Coach Lane should be considered, particularly with regard to the osteological paradox (Wood et al. 1992). However, given that many of the lesions recorded and interpreted at both sites were at least initiated during the first few years of life (e.g., enamel hypoplasia, rickets, scurvy, and cribra orbitalia), the comparison of the two different age-at-death profiles continues to have merit.
The presence of documented adults at Fewston has made it possible to gather the associated birth and death certificates, together with census records. This provides a known record of individuals who were born, lived, and died in Fewston and its environs—that is, the survivors. The skeletons of these adults do not show comparable levels of pathological lesions (e.g., cuspal enamel hypoplasia), and their stature does not appear to have been compromised; indeed, for males it was above the average stature for post-medieval England (177.3 cm for Fewston males and 160.4 cm for Fewston females) (Caffell and Holst 2017). One could argue that the children in the assemblage were non-survivors and that this is why they show a higher prevalence of pathology compared to the adults (Wood et al. 1992). Another hypothesis (mentioned above) is that these adolescents were not local to the area and instead represent migrants. This interpretation will be explored further after a more detailed comparison with Coach Lane.
North Shields was widely known to be a heavily industrialized, polluted, and insalubrious town in the nineteenth century (Proctor et al. 2016). The prevalence of metabolic, respiratory, and non-specific indicators of health stress at this site was high, as expected. In 1889 the British Medical Association estimated that vitamin D deficiency in the form of rickets in childhood was concentrated in the heavily industrialized areas of the northeast, where Coach Lane was located (Owen 1889). Vitamin D deficiency at this site is likely to have been exacerbated by the more northerly latitude, in conjunction with air pollution from the associated industries.
The high levels of vitamin D deficiency observed at Fewston, however, were not in keeping with historical records. John Snow, the famous nineteenth-century spatial epidemiologist, best known for his work on cholera, began his medical career as a doctor in a North Yorkshire village close to Fewston. Snow (1857) observed that rickets was a relatively rare disease in Yorkshire when compared to London. He attributed this to people from Yorkshire baking their own bread due to cheaper fuel sources, in contrast to Londoners who almost universally ate shop-bought bread, heavily adulterated with alum. Snow, like his contemporaries, believed that vitamin D deficiency was primarily dietary in origin, rather than due to a lack of sunlight, and he thought that alum was responsible for “weakening” the bones. The connection between sunlight and vitamin D deficiency was not made until the late nineteenth century, and diet was still thought to be the predominant cause of the disease even in the 1920s (see Findlay and Mellanby 1922). The key point here is that the prevalence of rickets at Fewston is contrary to Snow’s observations in North Yorkshire.
The prevalence rates of scurvy were also equally high in both the rural and urban sites studied here. It was expected that scurvy would be less prevalent in rural environments due to the increased availability of fruit and vegetables. A regional survey of diet and nutrition highlights that in rural Yorkshire the working classes ate largely bread, oatmeal, some sugar, and weak tea, rather than foods rich in vitamin C such as potatoes (Horrell and Oxley 2012). Historical records have also documented that the diet of women and children was more monotonous and less likely to include meat than the diet of men (Horrell and Oxley 2012; Humphries 2010).
Dental enamel hypoplasia (DEH) prevalence was comparable between the sites. DEH has multiple etiologies (e.g., infectious disease, trauma, malnutrition) and is generally regarded as a “non-specific” indicator of disease; however, it is worthwhile focusing on the type of hypoplastic defects present. While linear enamel hypoplasia is by far the most common form exhibited in skeletal samples generally, at Fewston there are a number of individuals that have “plane-form” and “pitted” defects of the type described by Ogden et al. (2007) as “cuspal enamel hypoplasia” (Fig. 9). This term describes the combination of pitted and plane-form lesions, together with a disruption in the pattern of the molar cusps, such that multiple small cusps form and develop. Ogden et al. (2007:960) noted a relatively high number of individuals with such defects (on deciduous and permanent teeth) from the post-medieval site of Broadgate in London and explored a range of reasons for these defects, including vitamin D deficiency. Pitting and cuspal enamel hypoplasia is also observed on the deciduous teeth at Fewston, indicating an in utero insufficiency. Purvis et al.’s (1973) clinical study noted an association between very similar hypoplastic lesions in the deciduous teeth and neonatal tetany, arising from deficiency in vitamin D in the mothers during the third trimester of pregnancy. Their sample was from Scotland, a northerly latitude, and they observed an increase in frequency during winter and spring when hours of sunshine were lowest. They also noted an association with increased maternal parity and low social status. Similar instances of modern cases of enamel hypoplasia associated with nutritional rickets have been reported in the more recent medical literature (e.g., Davit-Béal et al. 2014). The presentation of these defects is identical to those observed among the Fewston skeletons in terms of the teeth affected and location. Vitamin D deficiency in pregnant women is known to result in adverse maternal health and birth outcomes affecting the birth weight, bone mass, and immunity of the infant (Karras et al. 2016; Paterson and Ayoub 2015).

Figure 9. Cuspal enamel hypoplasia on teeth from Fewston.
An early-twentieth-century medical book by Dick (1922) focusing on the geographical distribution and clinical manifestations of rickets also describes dental lesions, which he argued to be pathognomonic of vitamin D deficiency as follows: “There may be only a pitting, producing a honeycombed appearance of the enamel, or the enamel covering is slight, and the cutting edge of the tooth presents sharp points, giving a characteristic appearance to the tooth” (1922:191–192). This description is again consistent with the dental lesions observed in some of the Fewston individuals. While it is easy to dismiss these early medical texts as outdated, particularly when published during a period in which the etiology of the condition was only poorly understood, it is important to give credit to the fact that these observations were made during a time when the disease was frequently encountered.
While enamel hypoplasia is generally considered to be a non-specific form of stress, in these instances it seems likely to have resulted from an insufficiency of vitamin D and/or calcium, beginning in utero and extending until 2 years of age. Vitamin D deficiency contributes to hypocalcaemia and hypophosphatemia, the latter of which is compounded by hyperparathyroidism brought about by hypocalcaemia (Foster et al. 2014:6–7). This lack of calcium and phosphorus results in developmental and mineralization defects in teeth via both direct and indirect mechanisms (Foster et al. 2014). It has been observed in clinical studies that vitamin D deficiency can result in inter-globular dentine, and this has been identified in archaeological teeth of individuals with residual rickets (D’Ortenzio et al. 2016). Future analysis of the Coach Lane site may benefit from a histological analysis of the teeth, but the Fewston skeletons have now been reburied. Of interest is that none of the adults from Coach Lane or Fewston exhibited evidence of cuspal enamel hypoplasia, indicating a strong association between these lesions and the risk of early mortality.
When interpreting the presence of pathological lesions and growth disruption early in the life course, it is important to consider the significance of maternal health for growth and immune status (Gowland 2015a). Maternal malnutrition, ill health, and exposure to toxins within the living or working environment during pregnancy will adversely affect the developing fetus. Intrauterine growth retardation is strongly associated with shorter height in childhood and adolescence (Chung and Kuzawa 2014). Furthermore, a mother who fails to meet her own genetic potential in growth is more likely to have an infant who is small for gestational age. Growth deficits early on in life can be difficult to recover from, particularly in adverse biolcultural environments (Chung and Kuzawa 2014). Indeed, the effects of a poor environment on growth could span multiple generations before it is fully reversed despite alleviation of environmental stressors (Barker 2012).
Finally, when interpreting palaeopathological evidence and delayed growth in terms of the local living environments, we must be sure that the pathological conditions observed in the skeletons of the children from Fewston and Coach Lane do in fact relate to the local area. With regard to this period of rapid industrialization and urbanization, migration is often conceptualized as unidirectional—from the countryside to towns. It is important to consider that during this period there was a significant amount of rural industry and that this led in some instances to the apprenticeship of urban children, who were removed to the countryside to work as laborers, as domestic servants, or in textile mills. These individuals were known as pauper apprentices: children taken from workhouses in cities, usually 10–12 years of age, and indentured to work far from their original home. The children worked long hours, 12 to 14 hours per day, and for no pay, but were instead “taught a trade” and were housed, fed, and given some education (Honeyman 2013; Levene 2010).
There was a flax mill at Fewston, known as Westhouse mill, and historical sources document the employment of pauper apprentices from the workhouses of Lambeth and Shoreditch in London, as well as elsewhere in England (Honeyman 2007). It therefore seems probable that this excess of adolescents at Fewston, with high frequencies of skeletal lesions and stunted growth, reflects a poor and destitute childhood in London rather than one spent at Fewston. Ives and Humphrey’s (2017) study of diaphyseal growth in children from the poor London parish of Bethnal Green during the nineteenth century also highlights severe growth deficits. Social status is one of the strongest determinants of health, and this was particularly evident in post-medieval England (Gowland 2018; Marmot and Wilkinson 2006). As discussed, the evidence for rickets and enamel hypoplasia at Fewston is consistent with the pathological evidence from the low-status post-medieval cemetery of Broadgate in London (Ogden et al. 2007; Pinhasi et al. 2006). The high prevalence of respiratory disease among these children at Fewston is also consistent with mill labor, in which pulmonary complaints, including byssinosis and tuberculosis, were a known occupational hazard (Wohl 1983). Further isotopic and archival investigation is currently being undertaken in order to verify the non-local origins of these adolescents (Gowland et al. 2017).
Conclusion
While the children at Coach Lane undoubtedly showed evidence of adverse living conditions in the form of poor skeletal growth and the presence of physiological insults to the skeleton, it was surprising and contrary to historical evidence that the children from the rural site showed comparable health deficits. One explanation is that we need to reevaluate our ideas of rural life during this time in terms of it providing a more beneficial living environment and diet. Alternatively, the health stress observed in some of the Fewston children may not relate to the local living environment at all but rather to an impoverished urban childhood in the workhouses of London and elsewhere. Childhood mobility during this period as well as urban-to-rural migration should be factored into our interpretations. Industry was not just an urban phenomenon but also a rural endeavor, and we should consider the impact of this on the health and population structure of Fewston. Finally, poverty has heritable biological consequences via poor maternal health status. This biological disadvantage then becomes exacerbated by poor working and living conditions. The Industrial Revolution was a period of relative social mobility, with a rise in the middle classes, but for the very poor and disenfranchised the inheritance of biological inequality in terms of morbidity and mortality risks, in addition to social disadvantage, meant that only the very tenacious could survive or thrive.
Acknowledgments
The authors would like to acknowledge the British Academy (SG132083) for funding this research. We would also like to thank Sally and Clive Robinson and the volunteers from the Washburn Heritage Centre for their contribution and support with the Fewston assemblage and Jenny Proctor at Pre-Construct Archaeology for access to the Coach Lane collection. I am very grateful to Paula Monguí for her translation of the abstract.
References Cited
Alred, David. 1997. Washburn Valley Yesterday: A Pictorial Record of Life in a Dales Valley. Smith Settle, Otley.
Arthur, Nichola A., Rebecca L. Gowland, and Rebecca C. Redfern. 2016. Coming of age in Britain: Osteological evidence for pubertal timing. American Journal of Physical Anthropology 159(4):698–713. DOI: 10.1002/ajpa.22929.
Barker, D. J. P. 2012. Developmental origins of chronic disease. Public Health 126(3):185–189. DOI: 10.1016/j.puhe.2011.11.014.
Bogin, Barry. 1999. Patterns of Human Growth. Cambridge University Press, Cambridge.
Brickley, Megan, and Rachel Ives. 2006. Skeletal manifestations of infantile scurvy. American Journal of Physical Anthropology 129(2):163–172. DOI: 10.1002/ajpa.20265.
Brickley, Megan, and Rachel Ives. 2008. The Bioarchaeology of Metabolic Bone Disease. Academic Press, London.
Brickley, Megan, and Adrian Miles. 1999. The Cross Bones Burial Ground, Redcross Way Southwark, London: Archaeological Excavations (1991–1998) for the London Underground Limited Jubilee Line Extension Project. MoLAS Monograph 3.
Brimblecombe, Peter. 1978. Air pollution in industrializing England. Journal of the Air Pollution Control Association 28(2):115–118. DOI: 10.1080/00022470.1978.10470577.
Buglass, John. 2009. The Church of St Michael and St Lawrence, Fewston, North Yorkshire: Interim Statement on the Archaeological Investigation. John Buglass Archaeological Services, on behalf of Washburn Heritage Group.
Burnett, John. 1984. Destiny Obscure: Autobiographies of Childhood, Education and Family from the 1820s to the 1920s. Penguin, London.
Caffell, Anwen. 2015. Transcription: Diary of John Dickinson, 1877 to 1912 (unpublished). Documents in private ownership (K. Dickinson and C. Monaghan).
Caffell, Anwen, and Malin Holst. 2017. Osteological Analysis: The Church of St Michael and St Lawrence, Fewston, North Yorkshire. Unpublished Report 1017, York Osteoarchaeology.
Chadwick, Edwin. 1842. Report on the Condition of the Labouring Population and on the Means of its Improvement. W. Clowes and Sons, London.
Chaudhary, Sunil, Namita Kalra, and Sunil Gomber. 2004. Tuberculous osteomyelitis of the mandible: A case report in a 4-year-old child. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 97(5):603–606. DOI: 10.1016/j.tripleo.2003.10.032.
Chung, Green C, and Christopher W. Kuzawa. 2014. Intergenerational effects of early life nutrition: Maternal leg length predicts offspring placental weight and birth weight among women in rural Luzon, Philippines. American Journal of Human Biology 26(5): 652–659. DOI: 10.1002/ajhb.22579.
Dalvin, Lauren A., and Wendy M. Smith. 2016. Orbital and external ocular manifestations of Mycobacterium tuberculosis: A review of the literature. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases 4:50–57. DOI: 10.1016/j.jctube.2015.11.001.
Davit-Béal, Tiphaine, Julie Gabay, Pauline Antoniolli, Jeanne Masle-Farquhar, and Maryse Wolikow. 2014. Dental complications of rickets in early childhood: Case report on 2 young girls. Pediatrics 133(4):e1077–e1081. DOI: 10.1542/peds.2013-0733.
Dawson, Heidi, and Kate Robson-Brown. 2012. Childhood tuberculosis: A probable case from late mediaeval Somerset, England. International Journal of Paleopathology 2(1):31–35. DOI: 10.1016/j.ijpp.2012.04.001.
DeWitte, Sharon N., Gail Hughes-Morey, Jelena Bekvalac, and Jordan Karsten. 2015. Wealth, health and frailty in industrial-era London. Annals of Human Biology 43(3):241–254. DOI: 10.3109/03014460.2015.1020873.
Dick, John Lawson. 1922. Rickets: A Study of Economic Conditions and Their Effects on the Health of the Nation. EB Treat & Co., New York.
D’Ortenzio, Lori, Isabelle Ribot, Emeline Raguin, Annabelle Schattmann, Benoit Bertrand, Bonnie Kahlon, and Megan Brickley. 2016. The rachitic tooth: A histological examination. Journal of Archaeological Science 74:152–163. DOI: 10.1016/j.jas.2016.06.006.
Elamin, Fadil, and Helen M. Liversidge. 2013. Malnutrition has no effect on the timing of human tooth formation. PLoS ONE 8:e72274.
Engels, Frederick. 1950. The Condition of the Working-Class in England in 1844: With a Preface Written in 1892. George Allen & Unwin Ltd, London.
Findlay, Leonard, and Edward Mellanby. 1922. Discussion on the etiology of rickets. British Medical Journal 2:836–858.
Foster, Brian L., Francisco H. Nociti, and Martha J. Somerman. 2014. The rachitic tooth. Endocrine Reviews 35(1):1–34. DOI: 10.1210/er.2013-1009.
Gaskell, Peter. 1833. The Manufacturing Population of England: Its Moral, Social and Physical Conditions and the Changes Which Have Arisen through the Use of Steam Machinery. Baldwin and Craddock, London.
Geber, Jonny. 2016. “Children in a ragged state”: Seeking a biocultural narrative of a workhouse childhood in Ireland during the Great Famine (1845–1852). Childhood in the Past 9:120–138. 10.1080/17585716.2016.1205344.
Goose, Nigel, and Katrina Honeyman. 2013. Introduction. In Childhood and Child Labour in Industrial England. Diversity and Agency, 1750–1914, edited by Nigel Goose and Katrina Honeyman. Ashgate, Surrey, pp. 1–22.
Gowland, Rebecca L. 2015a. Entangled lives: Implications of the developmental origins of health and disease (DOHaD) hypothesis for bioarcheology and the life course. American Journal of Physical Anthropology 158(4): 530–540. DOI: 10.1002/ajpa.22820.
Gowland, Rebecca L. 2015b. Review of Childhood and Child Labour in Industrial England. Childhood in the Past 8(1):68–70. DOI: 10.1179/1758571615Z.00000000028.
Gowland, Rebecca L. 2018. “A mass of crooked alphabets”: The construction and othering of working class bodies in industrial England. In Bioarchaeological Analyses and Bodies, edited by Pamela K. Stone. Springer, New York, pp. 147–163.
Gowland, Rebecca L., Anwen Caffell, Michelle Alexander, Leslie Quade, Andrew Millard, Malin Holst, Poppy Yapp, Chloe Brown. 2017. Indentured: Bioarchaeological Evidence for Pauper Apprentices in Nineteenth Century Yorkshire, England. Poster presented at the 86th Annual Meeting of the American Association of Physical Anthropologists, New Orleans. American Journal of Physical Anthropology Supplement, 162(S64):20.
Gowland, Rebecca L., and Sophie L. Newman. 2018. Children of the revolution: Childhood health inequalities and the life course during industrialisation of the 18th and 19th centuries in England. In Children and Childhood in the Past, edited by Patrick Beauchesne and Sabrina C. Agarwal. University of Florida Press, Gainesville, pp. 294–329.
Harker, Ronald. (ed) 1988. Timble Man: Diaries of a Dalesman. Hendon Publishing Co. Ltd, Lancashire.
Hillson, Simon. 1996. Dental Anthropology. Cambridge University Press, Cambridge.
Honeyman, Katrina. 2007. Child Workers in England, 1780–1820: Parish Apprentices and the Making of the Early Industrial Labour Force. Ashgate, Surrey.
Honeyman, Katrina. 2013. Compulsion, compassion and consent: Parish apprenticeship in early nineteenth-century England. In Childhood and Child Labour in Industrial England: Diversity and Agency, 1750–1914, edited by Nigel Goose and Katrina Honeyman. Ashgate, Surrey, pp. 71–96.
Horrell, Sara, and Deborah Oxley. 2012. Bringing home the bacon? Regional nutrition, stature, and gender in the industrial revolution. Economic History Review 65(4):1354–1379. DOI: 10.1111/j.1468-0289.2011.00642.x.
Hudson, Pat 1992. The Industrial Revolution. Arnold, London.
Humphries, Jane. 2010. Childhood and Child Labour in the British Industrial Revolution. Cambridge University Press, Cambridge.
Humphries, Jane. 2013. Care and cruelty in the workhouse: Children’s experiences of residential poor relief in eighteenth- and nineteenth-century England. In Childhood and Child Labour in Industrial England: Diversity and Agency, 1750–1914, edited by Nigel Goose and Katrina Honeyman. Ashgate, Surrey, pp. 115–134.
Ives, Rachel, and Louise Humphrey. 2017. Patterns of long bone growth in a mid-19th century documented sample of the urban poor from Bethnal Green, London, UK. American Journal of Physical Anthropology 163(1):173–186. DOI: 10.1002/ajpa.23198.
Karras, Spyridon N., Hana Fakhoury, Giovanna Muscogiuri, William B. Grant, Johannes M. van der Ouweland, Anna Maria Colao, and Kalliopi Kotsa. 2016. Maternal vitamin D levels during pregnancy and neonatal health: Evidence to date and clinical implications. Therapeutic Advances in Musculoskeletal Disease 8(4):124–135. DOI: 10.1177/1759720X16656810.
Kirby, Peter. 2013. Child Workers and Industrial Health in Britain, 1750–1850. Boydell Press, Woodbridge, UK.
Levene, Alysa. 2010. Parish apprenticeship and the old poor law in London. Economic History Review 63(4): 915–941.
Lewis, Mary E. 2002. Urbanisation and Child Health in Medieval and Post-Medieval England: An Assessment of the Morbidity and Mortality of Non-Adult Skeletons from the Cemeteries of Two Urban and Two Rural Sites in England (AD 850–1859). BAR British Series, 339. British Archaeological Reports, Oxford.
Lewis, Mary. 2004. Endocranial lesions in non-adult skeletons: Understanding their aetiology. International Journal of Osteoarchaeology 14(2):82–97. DOI: 10.1002/oa.713.
Lewis, Mary E. 2007. The Bioarchaeology of Children: Perspectives from Biological and Forensic Anthropology. Cambridge University Press, Cambridge.
Lewis, Mary. 2016. Work and the adolescent in medieval England (AD 900–1550): The osteological evidence. Medieval Archaeology 60 (1):138–171. DOI: 10.1080/00766097.2016.1147787.
Maresh, Marion M. 1955. Linear growth of long bones of extremities from infancy through adolescence: Continuing studies. American Journal of Diseases in Children 89(6):725–742. DOI: 10.1001/archpedi.1955.02050110865010.
Marmot, Michael, and Richard G. Wilkinson. 2006. Social Determinants of Health. 2nd ed. Oxford University Press, Oxford.
Matos, Vitor, and Ana Luísa Santos. 2006. On the trail of pulmonary tuberculosis based on rib lesions: Results from the human identified skeletal collection from the Museu Bocage (Lisbon, Portugal). American Journal of Physical Anthropology 130(2):190–200. DOI: 10.1002/ajpa.20309.
Mays, Simon, Megan Brickley, and Rachel Ives. 2006. Skeletal manifestations of rickets in infants and young children in a historic population from England. American Journal of Physical Anthropology 129(3):362–374. DOI: 10.1002/ajpa.20292.
Mays, Simon, Megan Brickley, and Rachel Ives. 2008. Growth in an English population from the industrial revolution. American Journal of Physical Anthropology 136(1):85–92. DOI: 10.1002/ajpa.20780.
Mays, Simon, Rachel Ives, and Megan Brickley. 2009. The effects of socioeconomic status on endochondral and appositional bone growth, and acquisition of cortical bone in children from 19th century Birmingham, England. American Journal of Physical Anthropology 140(3):410–416. DOI: 10.1002/ajpa.21076.
Moorrees, Coenraad F. A., Elizabeth A. Fanning, and Edward E. Hunt Jr. 1963a. Formation and resorption of three deciduous teeth in children. American Journal of Physical Anthropology 21:205–213. DOI: 10.1002/ajpa.1330210212.
Moorrees, Coenraad F. A., Elizabeth A. Fanning, and Edward E. Hunt Jr. 1963b. Age variation of formation stages for ten permanent teeth. Journal of Dental Research 42(6):1490–1502.
Newman, Sophie L., and Rebecca L. Gowland. 2015. Brief communication: The use of non-adult vertebral dimensions as indicators of growth disruption and non-specific health stress in skeletal populations. American Journal of Physical Anthropology 158(1):155–164. DOI: 10.1002/ajpa.22770.
Newman, Sophie L., and Rebecca L. Gowland. 2016. Dedicated followers of fashion? Bioarchaeological perspectives on socio-economic status, inequality, and health in urban children from the Industrial Revolution (18th–19th C), England. International Journal of Osteoarchaeology 27(2):217–229. DOI: 10.1002/oa.2531.
Ogden, Alan. 2008. Advances in the palaeopathology of teeth and jaws. In Advances in Human Palaeopathology, edited by Ron Pinhasi and Simon Mays. Wiley, New York, pp. 282–307.
Ogden, Alan R., Ron Pinhasi, and William J. White. 2007. Gross enamel hypoplasia in molars from subadults in a 16th–18th century London graveyard. American Journal of Physical Anthropology 133(3):957–966. DOI: 10.1002/ajpa.20608.
Ortner, Donald J. 2003. Identification of Pathological Conditions in Human Skeletal Remains. Academic Press, New York.
Ortner, Donald J., and Simon Mays. 1998. Dry bone manifestations of rickets in infancy and early childhood. International Journal of Osteoarchaeology 8(1):45–55. DOI: 10.1002/(SICI)1099-1212(199801/02)8:1<45::AID-OA405>3.0.CO;2-D.
Owen, Isambard. 1889. Geographical distribution of rickets, acute and subacute rheumatism, chorea, cancer, and urinary calculus in the British Islands. The British Medical Journal 1464 (1): 111–116.
Paterson, Colin R., and David Ayoub. 2015. Congenital rickets due to vitamin D deficiency in mothers. Clinical Nutrition 34:793–798. DOI: 10.1016/j.Clnu.2014.12.006.
Pinchbeck, Ivy, and Margaret Hewitt. 1973. Children in English Society, Volume 2, From the Eighteenth Century to the Children Act, 1948. Routledge, London.
Pinhasi, Ron, P. Shaw, Bill White, and Alan R. Ogden. 2006. Morbidity, rickets and long-bone growth in post-medieval Britain—A cross-population analysis. Annals of Human Biology 33(3):372–389. DOI: 10.1080/03014460600707503
Proctor, Jennifer, Märit Gaimster, and James Young Langthorne. 2016. A Quaker Burial Ground at North Shields: Excavations at Coach Lane, Tyne and Wear.Pre-construct Archaeology Monograph Series, London.
Purvis, R. J., W. J. McBarrie, G. S. MacKay, E. M. Wilkinson, F. Cockburn, and N. R. Belton. 1973. Enamel hypoplasia of the teeth associated with neonatal tetany: A manifestation of maternal vitamin D deficiency. The Lancet 302:811–814.
Reports from the Commissioners on Conditions in Factories, 1833, vol XXI, parliamentary papers.
Roberts, Charlotte A., Anwen Caffell, Kori L. Filipek-Ogden, Rebecca Gowland, and Tina Jakob. 2016. “Til poison phosphorous brought them death”: A potentially occupationnally-related disease in a post-medieval skeleton from north-east England. International Journal of Paleopathology 13:39–48. DOI: 10.1016/j.ijpp.2015.12.001.
Roberts, Charlotte A., and Brian Connell. 2004. Guidance on recording palaeopathology. In Guidelines to the Standards for Recording Human Remains, edited by Megan Brickley and Jacqueline I. McKinley. IFA Paper No. 7, BABAO and IFA, Reading, UK, pp. 34–39.
Roberts, Charlotte A., and Keith Manchester. 2005. The Archaeology of Disease. The History Press, Stroud.
Second Report of the Commissioners. 1845. The State of Large Towns and Populus Districts, Vol. 2. William Clowes and Sons, London.
Santos, Ana Luísa, and Charlotte A. Roberts. 2001. A picture of tuberculosis in young Portugese people in the early 20th century: A multidisciplinary study of the skeletal and historical evidence. American Journal of Physical Anthropology 115(1):38–49. DOI: 10.1002/ajpa.1054.
Santos, Ana Luísa, and Charlotte A. Roberts. 2006. Anatomy of a serial killer: Differential diagnosis of tuberculosis based on rib lesions of adult individuals from the Coimbra Identified skeletal collection, Portugal. American Journal of Physical Anthropology 130(1):38–49. DOI: 10.1002/ajpa.20160.
Saunders, Shelley R. 2008. Juvenile skeletons and growth-related studies. In Biological Anthropology of the Human Skeleton, edited by M. Anne Katzenberg and Shelley R. Saunders. Wiley-Liss, New York, pp. 117–147.
Scheuer, Louise, and Sue Black. 2000. Developmental Juvenile Osteology. Academic Press, London.
Shameem, Mohammad, Talha Saad, Rakesh Bhargava, Zuber Ahmad, Nazish Fatima, Haris Khan, and Fakhrul Huda. 2009. Frontal bone tuberculosis presenting with blindness in a 14-year-old girl: A case report. Journal of Medical Case Reports 3:8220. DOI: 10.4076/1752-1947-3-8220.
Shapland, Fiona, and Mary E. Lewis. 2013. Brief communication: A proposed osteological method for the estimation of pubertal stage in human skeletal remains. American Journal of Physical Anthropology 151(2):302–310. DOI: 10.1002/ajpa.22268.
Shapland, Fiona, and Mary E. Lewis. 2014. Brief communication: A proposed method for the assessment of pubertal stage in human skeletal remains using cervical vertebrae maturation. American Journal of Physical Anthropology 153(1):144–153. DOI: 10.1002/ajpa.22416.
Sheikh, Soheyl, S. Pallagatti, Deepak Gupta, and Amit Mittal. 2012. Tuberculous osteomyelitis of mandibular condyle: A diagnostic dilemma. Dentomaxillofacial Radiology 41:169–174. DOI: 10.1259/dmfr/56238546.
Smith, B. Holly. 1991. Standards of human tooth formation and dental age assessment. In Advances in Dental Anthropology, edited by Marc A. Kelley and Clark Spencer Larsen. Wiley-Liss, New York, pp. 143–168.
Snow, John. 1857. On the adulteration of bread as a cause of rickets. Lancet 2, 1766:4–5.
Stark, Robert J. 2014. A proposed framework for the study of palaeopathological cases of subadult scurvy. International journal of Palaeopathology 5:18–26. DOI: 10.1016/j.ijpp.2014.01.005.
Stuart-Macadam, Patricia. 1991. Anaemia in Roman Britain. In Health in Past Societies: Biocultural Interpretations of Human Remains in Archaeological Contexts, edited by Helen Bush and Marek Zvelebil. BAR International Series, 567. Tempus Reparatum, British Archaeological Reports, Oxford, pp. 101–113.
Wilkes, Sue. 2011. The Children History Forgot: Young Workers of the Industrial Age. Robert Hale, London.
Wohl, Anthony S. 1983. Endangered Lives: Public Health in Victorian England. Harvard University Press, Cambridge.
Wood, James W., George R. Milner, Henry C. Harpending, and Kenneth M. Weiss. 1992. The osteological paradox: Problems of inferring prehistoric health from skeletal samples. Current Anthropology 33(4):343–370. DOI: 10.1086/204084.
Young, George Malcolm, and W. D. Handcock. 1956. English Historical Documents, Vol. 12, Pt. 1, 1833–1874. Eyre & Spottiswoode, London.
1. In addition to the listed reference, an abridged version of this diary was published: Harker, R (ed) 1988. Timble Man: Diaries of a Dalesman (Nelson, Lancashire).
Supplemental Tables
Table S1. Coach Lane: dental enamel hypoplasia (DEH; pitting, lines, and grooves).
|
Age Group |
Deciduous |
Permanent |
All Teeth |
|||||||||||||||||
|
DEH |
Total |
% |
DEH |
Total |
% |
DEH |
Total |
% |
||||||||||||
|
Foetus |
< 36w |
— |
0 |
— |
— |
0 |
— |
— |
0 |
— |
||||||||||
|
Neonate |
36w–1m |
0 |
34 |
0.00 |
— |
0 |
— |
0 |
34 |
0.0 |
||||||||||
|
Infant |
1–12m |
13 |
128 |
10.2 |
0 |
3 |
0.0 |
13 |
131 |
9.9 |
||||||||||
|
Young Juvenile |
1–5.9y |
61 |
382 |
16.0 |
27 |
108 |
25.0 |
88 |
490 |
18.0 |
||||||||||
|
Older Juvenile |
6–11.9y |
8 |
45 |
17.8 |
37 |
108 |
34.3 |
45 |
153 |
29.4 |
||||||||||
|
Adolescent |
12–19.9y |
— |
0 |
— |
114 |
243 |
46.9 |
114 |
243 |
46.9 |
||||||||||
|
Total |
82 |
589 |
13.9 |
178 |
462 |
38.5 |
260 |
1,051 |
24.7 |
|||||||||||
Table S2. Coach Lane: cuspal enamel hypoplasia (CEH).
|
Age Group |
Deciduous |
Permanent |
All Teeth |
|||||||||||||||||
|
CEH |
Total |
% |
CEH |
Total |
% |
CEH |
Total |
% |
||||||||||||
|
Foetus |
< 36w |
— |
0 |
— |
— |
0 |
— |
— |
0 |
— |
||||||||||
|
Neonate |
36w–1m |
0 |
34 |
0.0 |
— |
0 |
— |
0 |
34 |
0.0 |
||||||||||
|
Infant |
1–12m |
0 |
128 |
0.0 |
1 |
3 |
33.3 |
1 |
131 |
0.8 |
||||||||||
|
Young Juvenile |
1–5.9y |
2 |
382 |
0.5 |
3 |
108 |
2.8 |
5 |
490 |
1.0 |
||||||||||
|
Older Juvenile |
6–11.9y |
0 |
45 |
0.0 |
0 |
108 |
0.0 |
0 |
153 |
0.0 |
||||||||||
|
Adolescent |
12–19.9y |
— |
0 |
— |
0 |
243 |
0.0 |
0 |
243 |
0.0 |
||||||||||
|
Total |
2 |
589 |
0.3 |
4 |
462 |
0.9 |
6 |
1,051 |
0.6 |
|||||||||||
Table S3. Fewston: dental enamel hypoplasia (DEH; pitting, lines, and grooves).
|
Age Group |
Deciduous |
Permanent |
All Teeth |
|||||||||||||||||
|
DEH |
Total |
% |
DEH |
Total |
% |
DEH |
Total |
% |
||||||||||||
|
Foetus |
< 36w |
— |
0 |
— |
— |
— |
— |
— |
0 |
— |
||||||||||
|
Neonate |
36w–1m |
— |
0 |
— |
— |
0 |
— |
— |
0 |
— |
||||||||||
|
Infant |
1–12m |
0 |
7 |
0.0 |
0 |
1 |
0.0 |
0 |
8 |
0.0 |
||||||||||
|
Young Juvenile |
1–5.9y |
12 |
131 |
9.2 |
16 |
112 |
14.3 |
28 |
243 |
11.5 |
||||||||||
|
Older Juvenile |
6–11.9y |
6 |
67 |
9.0 |
53 |
247 |
21.5 |
59 |
314 |
18.8 |
||||||||||
|
Adolescent |
12–19.9y |
— |
3 |
— |
111 |
455 |
24.4 |
111 |
458 |
24.2 |
||||||||||
|
Total |
18 |
208 |
8.7 |
180 |
815 |
22.1 |
198 |
1023 |
19.4 |
|||||||||||
Table S4. Fewston: cuspal enamel hypoplasia (CEH).
|
Age Group |
Deciduous |
Permanent |
All Teeth |
|||||||||||||||||
|
CEH |
Total |
% |
CEH |
Total |
% |
CEH |
Total |
% |
||||||||||||
|
Foetus |
< 36w |
— |
— |
— |
— |
— |
— |
— |
0 |
— |
||||||||||
|
Neonate |
36w–1m |
— |
0 |
— |
— |
0 |
— |
— |
0 |
— |
||||||||||
|
Infant |
1–12m |
0 |
7 |
0.0 |
0 |
1 |
0.0 |
0 |
8 |
0.0 |
||||||||||
|
Young Juvenile |
1–5.9y |
0 |
131 |
0.0 |
0 |
71 |
0.0 |
0 |
202 |
0.0 |
||||||||||
|
Older Juvenile |
6–11.9y |
1 |
67 |
1.5 |
12 |
271 |
4.4 |
13 |
338 |
3.8 |
||||||||||
|
Adolescent |
12–19.9y |
0 |
3 |
0.0 |
28 |
472 |
5.9 |
28 |
475 |
5.9 |
||||||||||
|
Total |
1 |
208 |
0.5 |
40 |
815 |
4.9 |
41 |
1,023 |
4.0 |
|||||||||||