
Bioarchaeology International
Volume 8, Numbers 3–4: 182–215
DOI: 10.5744/bi.2023.0004
Received 25 January 2023
Revised 23 September 2023
Accepted 7 December 2023
Forgotten Children: The Fetal and Infant Skeletal Remains of the W. D. Trotter Anatomy Museum, New Zealand
Megan Southorn,#,a Siân E. Halcrow,#,*,a Stephie R. Lončar,a Emma L. Sudron,a,b Chris Smith,a and D. Gareth Jonesa
ABSTRACT Fetal and infant skeletal remains in anatomical collections remain an underutilized yet important source of information on the interactions of gender, class, and religion during pregnancy and infant loss. The W. D. Trotter Anatomy Museum at the University of Otago in New Zealand, founded in the nineteenth century, houses more than 2,000 models and anatomical “specimens,” with many of the skeletal remains lacking provenience information. This research aimed to both provide an inventory of the fetal and infant skeletal remains and identify through archival analysis the social context of those whose remains were obtained by the museum. An osteological analysis was carried out to assess the minimum number of individuals (MNI), estimate age-at-death, and provide evidence for pathology and dissection. The results are interpreted in the context of the archival accession data and historical information at the time to provide the social context in which these people lived and therefore information that may be related to their deaths and acquisition of their bodies by the university. Most of the infants within the collection died around the time of full-term birth, and some individuals have evidence for developmental pathology, birth trauma, and/or postmortem dissection. The historical context and legislation around body donation suggests structural inequality played a role in the acquisition of these infants’ remains from mothers (primarily poor and/or unmarried women) and that these remains went through a process of commodification and objectification and were retained as developmental teaching “specimens” and examples of pathology.
Keywords: Anatomy Museum; infant osteology; structural violence
GERMAN Skelettüberreste von Föten und Säuglingen in anatomischen Sammlungen sind nach wie vor eine wenig genutzte, aber wichtige Informationsquelle über die Wechselwirkungen von Geschlecht, soziale Schicht und Religion während der Schwangerschaft und beim Verlust des Kindes. Das im 19. Jahrhundert gegründete W. D. Trotter Anatomy Museum an der University of Otago in Neuseeland beherbergt mehr als 2000 Exponate und anatomische „Präparate“, wobei es bei vielen Skelettüberresten keine Angaben zur Herkunft gibt. Ziel dieser Forschung war es, sowohl eine Bestandsaufnahme der Skelettüberreste von Föten und Säuglingen zu erstellen als auch durch eine Archivanalyse den sozialen Kontext derjenigen zu identifizieren, deren Überreste vom Museum erhalten wurden. Es wurde eine osteologische Analyse durchgeführt, um die Mindestanzahl der Personen (MNI) zu ermitteln, das Sterbealter abzuschätzen und Hinweise auf Pathologie und Sektion/Obduktion zu geben. Die Ergebnisse werden im Kontext der archivierten Zugangsdaten und historischen Informationen zu der Zeit interpretiert, um den sozialen Kontext zu ermitteln, in dem diese Menschen lebten, und damit Informationen, die mit ihrem Tod und dem Erwerb ihrer Körper durch die Universität in Zusammenhang stehen könnten. Die meisten Säuglinge in der Sammlung starben etwa zum Zeitpunkt der Geburtsreife, und bei einigen Personen liegen Hinweise auf Entwicklungsstörungen, Geburtstrauma und/oder eine postmortale Obduktion vor. Der historische Kontext und die Gesetzgebung zur Körperspende legen nahe, dass strukturelle Ungleichheit beim Erwerb der Überreste dieser Säuglinge von Müttern (hauptsächlich arme und/oder unverheiratete Frauen) eine Rolle gespielt hat und dass diese Überreste einen Prozess der Kommerzialisierung und Objektivierung durchlaufen haben und als solche aufbewahrt wurden Entwicklungslehre-„Präparate“ und Exponate der Pathologie.
Translation by: Stephie Lončar and Sara Otto
SCOTTISH GAELIC Tha fuighill cnàimhneach leatrom anabaich is leanaban ann an cruinneachaidhean anatomach fhathast nan stòras fiosrachaidh nach eilear a’ cleachdadh gu leòr ach a tha cudromach a thaobh fiosrachaidh air eadar-obrachadh gnè, clas, agus creideamh tro leatromachd agus call leanaban. Ann an Taigh-tasgaidh Anatomy WD Trotter aig Oilthigh Otago ann an Sealan Nuadh, a chaidh a stèidheachadh san naoidheamh linn deug, tha còrr air 2000 modal agus ‘sampaill’ anatomach, le mòran de na fuighill cnàimhneach gun fhiosrachadh air tùs. Bha an rannsachadh seo ag amas air an dà chuid cunntas a thoirt air na fuighill cnàimhneach leatrom anabaich is pàiste a bh’ aig an oilthigh agus sealltainn, tro sgrùdadh tasglainn, an co-theacsa sòisealta. Chaidh mion-sgrùdadh osteologach a dhèanamh gus measadh a dhèanamh air an àireamh as lugha de leanabain fa-leth (MNI), tuairmse air aois-aig-bàis, agus fianais airson eòlas-ghlar agus gearradh na mhìrean. Tha na toraidhean air am mìneachadh ann an co-theacsa dàta sealbhachaidh tasglainn agus fiosrachadh eachdraidheil aig an àm gus an co-theacsa sòisealta anns an robh na leanabain beò a thoirt seachad, agus, mar sin, fiosrachadh a dh’ fhaodadh a bhith co-cheangailte ri am bàs agus mar a fhuaireadh na cuirp aca leis an oilthigh. Bhàsaich a’ mhòr-chuid de na naoidheanan taobh a-staigh a’ cho-chruinneachaidh aig àm breith làn-ùine, agus tha fianais aig cuid aca air eòlas-ghalair leasachaidh, trauma breith agus / no gearradh post-mortem. Tha an co-theacsa eachdraidheil agus an reachdas mu thabhartas bodhaig a’ nochdadh gun robh pàirt aig neo-ionannachd structarail ann a bhith a’ faighinn fuighill nan leanaban bho mhàthraichean (boireannaich a bha bochd agus/no gun phòsadh sa mhòr-chuid), agus gun deach na fuighill sin tro phròiseas bathair agus dìmeas agus gun deach an cumail mar ‘sampaill’ leasachadh teagasg agus eisimpleirean de eòlas-ghalar.
Translation by: Annella Macarthur
Dedicated to the babies lost and subsequently kept in the W. D. Trotter Museum, whose life stories (albeit short) we hope to give a voice at least partially to here.
The study of historic human remains themselves provides vital information on the life experiences of past individuals and populations (Larsen 2015). Although the lives of individuals in more recent history are better documented than the lives of earlier populations, specific subgroups of society are often forgotten in these narratives (i.e., women, children, the poor, disabled or mentally ill) (Clarke 2012; Helleiner et al. 2001; Riley 1988). Historical anatomical human remains are a unique source of information to assess the life experiences of individuals and communities in the past, and the study of infant remains from these contexts may give us an understanding of the development of medicalization of the body during pregnancy and childbirth (Dittmar and Mitchell 2016, 2018; Muller and Butler 2018). Due to the close physiological relationship between mothers and infants during pregnancy and breastfeeding, pathology that exists in fetal and infant skeletal remains can be evidence for nutritional deficiencies and infectious disease in mothers (Gowland and Halcrow 2020).
With the shift toward anatomy becoming a more humanistic field, ignoring the social power structures and sociocultural context that led to these individuals being anatomized and held in collections is no longer acceptable (de la Cova 2019; Muller et al. 2017; Muller and Butler 2018). Such studies may lend insight into the influences that led to them being anatomized, such as disparities in access to health care historically and the inequitable treatment of the dead. Perspectives on the acquisition and use of human remains, their contribution to anatomy and biological anthropology, and acknowledgment of their history of acquisition have changed over time within the museum and anthropological contexts (Alberti 2011; Claes and Deblon 2018; Wilson 2015). The use and display of these remains can be conceptualized through the lens of the commodification of bodies for their continued use in medical teaching and as objects of curiosity, including for the display and voyeurism of individuals with pathology (Claes and Deblon 2018; Hodge 2013; Ion 2022; MacDonald 2012).
Galtung (1969), who was the primary proponent of the theoretical model of structural violence, defined this as a way in which social structures, laws, and other social institutions cause harm to individuals and prevent groups of people from meeting their full potential through the deprivation of basic needs through social forces of power. The amassing of anatomical skeletal collections has been understood through this theoretical model, with many works evoking this lens in the context of the treatment of the African American bodies in anatomical and anthropological contexts (e.g., de la Cova 2019; Lans 2020; Nystrom 2014; Watkins 2018; Watkins and Muller 2015). Like the United States and United Kingdom, in New Zealand, the change of legislation in the nineteenth century to reduce the incentive for graverobbing led to the legal right for the acquisition of bodies from public institutions by physicians (Anatomy Act 1875). Research on these historical anatomical collections highlights social deprivation related to factors such as race and poverty that were central to the formation of these collections (de la Cova 2011; Jones and Whitaker 2012; Lans 2021; Richardson 1987; Sappol 2002). The very presence of vulnerable or marginalized individuals such as infants within an anatomical collection can be indicative of the structural violence they (and their parent/s) experienced during their short lives and after death (Zuckerman 2021). It has been suggested that most of the cadavers of adults received by the University of Otago Medical School historically were likely unclaimed bodies from hospitals, societies for the poor, and an asylum, all of whom cared for or housed society’s most vulnerable, those who faced societal structures that harmed them throughout their lives and after death (Jones and Fennell 1991).
We acknowledge the sensitive nature of this study of these fetal and infant remains (Beiter et al. 2019; Biers 2020; Bonney et al. 2020; Fourniquet et al. 2019; Squires and Piombino-Mascali 2022; Wilson 2015), both from the perspective of how they may have been acquired in the past and our reflections on the ethics of those practices today, and the potential to continue and compound this injustice through the osteological investigation and objectification of these infants. Part of our intention here is to study the osteology and pathology of these infants to start to tell the stories of their (albeit) short lives and the experiences of their parents and to attempt to understand something about how they came to be in these collections. This analysis helps with elucidating the context of provenience, which is important when considering their use in teaching, research, and display and informing students and researchers (Cormer 2022; Hildebrandt 2019). From a scientific paleopathological point of view, images are expected for verification of the observations. However, we are cognizant that these photographs could be disturbing for some and may be seen as objectification and continuation of this structural violence and inequitable treatment of these remains. We also recognize the personal sensitive nature of fetal and infant loss for some and the social taboo surrounding discussing and engaging with pregnancy loss (Cox 2019). Therefore, we include the images of the infants as supplementary information, so if readers wish to refer to these, they have agency in their decision.
Infants in anatomical education
Literature on the role of the fetus and infant in anatomical education is sparse (e.g., Armüller and Lenk 2022; Dittmar and Mitchell 2016; Wilson 2015). The nineteenth and twentieth centuries were a formative time for anatomy and the collection of humans for their dissection and curation. In the United Kingdom, adult males were the preferred body for most dissections during the nineteenth century (Dittmar and Mitchell 2016), and for that reason, literature that focuses on the use of the human body in medical education largely ignores women, infants, and children. The primary reason male cadavers were preferred in medical education in the United Kingdom and other countries was their availability. Under the Act for Regulating Schools of Anatomy 1832 (United Kingdom), bodies legally available for dissection were either executed felons or those who had died in workhouses, hospitals, or other charitable institutions who had no family to claim their body for burial or cremation. Although this law meant that the bodies of women and children’s bodies were legally available for dissection, their availability was restricted by the wardens of such charitable institutions. These wardens were known to refuse to hand over custody of women’s bodies to anatomists after death (Dittmar and Mitchell 2018) or would refuse to admit pregnant people into their care entirely (Clarke 2012; Dittmar and Mitchell 2018). Pregnant bodies from executions were also largely unavailable as their execution was incredibly rare: all pregnant people destined for the gallows were given a stay of execution until after the birth of their child (Dittmar and Mitchell 2018), thus rendering the bodies nearly completely unavailable to anatomists through that means. Evidence from other skeletal collections around the globe suggests that the rarity and importance of these bodies in obstetric education has been a major incentive for the continued holding of the remains in museums for future generations (Dittmar and Mitchell 2016; Kosenko et al. 2022). Interestingly, in the New Zealand context, the bodies of (likely not pregnant) women were readily made available for use in anatomy education at the University of Otago from institutions such as Seacliff Lunatic Asylum (Jones 2012) and in at least one case from the “gaol” (jail) (Sudron 2021).
As discussed, historical legislation in Great Britain meant that dissection was largely limited to criminals and impoverished adults (mostly men), making the presence of infants and perinates in a museum even more unusual (Dittmar and Mitchell 2016; Jones and Fennell 1991; Richardson 1987). Dissection or dismemberment of the body after death went against the Christian beliefs of the time, where in order to be resurrected when Christ returned to Earth, the physical body needed to remain intact (Knight 2018; Zuckerman et al. 2021). Therefore, the donation of remains of a newborn or an infant to a museum is an unusual and unexpected choice for Victorian and Edwardian era parents in a predominantly Christian society such as historic Dunedin. More pragmatic justifications as to why these infant remains may have ended up in the care of the university, such as avoiding the cost of burial or religious doctrine preventing the burial of unbaptized infants in consecrated ground (Dine 2019; Murphy 2011), are also problematic. Across Dunedin, there are many historic stillbirths and infants buried in cemetery plots of all classes. For instance, the Northern Cemetery, one of Dunedin’s largest cemeteries, was secular and contained a large number of council owned “third-class” plots open for the burial of those who could not afford to purchase a plot themselves (Lane 2018). The University of Otago Medical School likely acquired the remains of fetuses and infants as the only reliable way of studying early human development at the time. What is not clear, however, is the social context that led to the donation or forced acquisition of the infant remains for retention in the museum.
The main aim of this research is to both provide an inventory of the fetal and infant skeletal remains and identify through archival analysis the social context of those whose remains were obtained and held in the W. D. Trotter Anatomy Museum. To do this, we completed an osteological analysis of the remains and undertook archival research to investigate the social and historical circumstances for the inclusion of fetal and infant remains in this anatomical collection, including medical approaches to childbirth and consent to dissection for the purposes of medical education. There has been a growing awareness of the continuing impact of the profound lack of ethical standards in the collection, curation, and use of human skeletal remains for research and teaching purposes. An investigation of the rich social and historical context and ethics of past acquisition practices of historical anatomical collections in institutions is integral to starting this process of ethically engaging with these collections (Adams 2009). The historical collecting practices define, in most part, what remains are held within museums today as guided by what was seen as acceptable in their social and historic context. Fetal, infant, and child remains in these collections pose several ethical issues, and it is important to understand the historical acquisition and provenance for the consideration of their use in teaching, research, and display today (Wilson 2015).
The W. D. Trotter Anatomy Museum, University of Otago in Dunedin
This museum was founded in the late 1870s as part of the Medical School and houses more than 2,000 human and model anatomical "specimens" used in education and research. In the museum is a collection of fetal and infant skeletal remains. No prior osteological or historical archival analyses had been completed on these infant remains.
The city of Dunedin was founded in 1848 by Scottish colonial settlers, and the university was established less than 30 years later, in 1869. The land for the Dunedin settlement had been purchased from the local iwi (tribe) of Kāi Tahu (Carmalt Jones 1945), and the subsequent discovery of gold inland from Dunedin in 1861 made the city the industrial, financial, and commercial center of New Zealand, a fine city to found New Zealand’s first university (Carmalt Jones 1945; Hercus and Bell 1964; Trapeznik 2011).
Methods
Age definitions
All skeletonized infants (age-at-death of less than one year) in the W. D. Trotter Museum collection were analyzed, and all historical information pertaining to infants acquired by the University of Otago Medical School for dissection was included in this project. We refer to these individuals collectively as “infants,” in line with the World Health Organization definition of the first year of life. Other definitions used in this research are “fetus”, aged up to 37 weeks gestation; “perinate,” from birth to the seventh day of life; “neonate,” from the eighth to twenty-eighth day of life; and “post-neonate,” from the twenty-ninth day of life to the end of the first year. The term “fetus” is used in bioarchaeology to refer to an individual older than eight weeks gestation but not yet born (Lewis 2007). We have used the term “fetus” in this research to refer to an individual aged prior to when a pregnancy reaches “term” at the end of the thirty-seventh week of gestation, because any individual older than 37 weeks of gestation may well have been born before their death and therefore cross the line of live birth that marks the transition from “fetus” to “perinate.” All other definitions are concurrent with bioarcheological and clinical literature (Halcrow 2017; Halcrow and Tayles 2008; Lewis 2007).
Historical archival analysis
Available diaries, letters, and other forms of communication between undertakers, hospitals, medical practitioners, and university were investigated via an extensive search of materials associated with the Anatomy Department within the Hākena database. No mention of procurement of infant remains for use in anatomy was found from those sources.
The primary archival text for this study was The Register of Anatomical Material, which was supplemented with historic undertaker records from Hugh Gourley Ltd. (now Gillions Funeral Services). We obtained the historical death certificates from the New Zealand Department of Internal Affairs. The information obtained from these resources is described in Table 1 and below. A review of relevant historical literature and primary historical (archival) sources was used to identify any information available on when and why these remains may have been acquired, why they died, and to assess how aspects of gender, class, religion, and the concept of personhood may have interacted to result in the curation of these within the W. D. Trotter Anatomy Museum.
The University of Otago Register of Anatomical Material
This archival book documents the acquisition of bodies by the Department of Anatomy from the period of 1876–1941 and is held in the Hocken Collection | Uare Taoka o Hākena in Dunedin (Fig. 1). It is assumed that all bodies used in anatomy education at the University of Otago in this period were listed in this register. The register listed the name of the deceased, their age-at-death, the date the university received their body, the date any dissection commenced, the institution it was received from, the cause of death, the undertaker, the date of burial (if this occurred), any injections they received (e.g., to help with preservation), and any extra notes. Interestingly, in the case of infants, instead of indicating the same undertaker was used for burial “do,” often a dash was written instead.
The entire register was read systematically, taking photographs of each entry for an infant. This information was then digitally transcribed into a Microsoft Excel spreadsheet. At Gillions Funeral Services, which recorded many of the early body donations to the University of Otago (see Supplementary File 1), we assessed the ledgers from 1876–1941 (as this was the period documented in the University of Otago Register of Anatomical Material), using the index to find all cases of bodies that were sent to the University of Otago by Hugh Gourley Ltd. We then cross-referenced the data from the Hocken Collection | Uare Taoka o Hākena, recording any instances of infants being sent to the Medical School and recording any extra information about the infants noted in the Register of Anatomical Material. Examples of this included costs associated with “supplying” the body of these individuals to the university and the date when dissection was commenced.
Hugh Gourley Ltd. Funeral Services Ledgers
The ledgers date from 1875, when the business was known as Hugh Gourley Ltd., to the present day (now Gillions Funeral Services). As Gourley was one of the two primary undertakers in the Dunedin region, it provides a representative insight into the context of individuals who were sent to the university. The earlier ledgers were up to 500 pages long, with each book covering up to five years of finances for the funeral home. The books recorded the name of the individual being buried (or the person footing the bill in some cases), if the person was being buried by a trust, what funeral services they requested, place of death, sometimes date of death or burial, and any costs incurred. Each ledger had an index book of surnames or company names that indicated the page in which their transactions with Gourley Ltd. were listed. An example of this is provided in Supplementary Figure 1. Institutions such as the Dunedin Public Hospital and the University of Otago regularly had complete pages devoted to the bodies Gourley was involved with undertaking, as shown in Supplementary Figure 2. The earlier historic entries were typically more detailed regarding place and context of death.
Table 1. Historical Archival Accession Sources
|
Archival Sources |
Source |
Information Included |
|
The Register of Anatomical Material |
Hocken Collection | Uare Taoka o Hākena in Dunedin |
Acquisitions of human remains from 1876–1941 includes name of the deceased, their age at death, the date the university received their body, the date any dissection commenced, the institution from which it was received, the cause of death, the undertaker, the date of burial (if this occurred), any injections they received (e.g., to help with preservation), and any extra notes. |
|
Hugh Gourley Ltd. |
Gillions Funeral Home, private collection, Dunedin |
Name of the individual being buried (or the person footing the bill in some cases), if the person was being buried by a trust, what funeral services they requested, place of death, sometimes date of death or burial, and any costs incurred (for example, for transport of the body). |
|
Historical Death Certificates |
New Zealand Department of Internal Affairs | Te Tari Taiwhenua (NZDIA) The online historical search (https://www.bdmhistoricalrecords.dia.govt.nz/) was used to find the registration number for historical records to be ordered from NZDIA. |
Cause of death, date of death, age-at-death, parental marital status, father’s occupation, burial location, date of burial, and name of medical professional who attended illness and death. |
Figure 1. University of Otago Register of Anatomical Material (with permission from the Hocken Collections | Uare Taoka o Hākena).
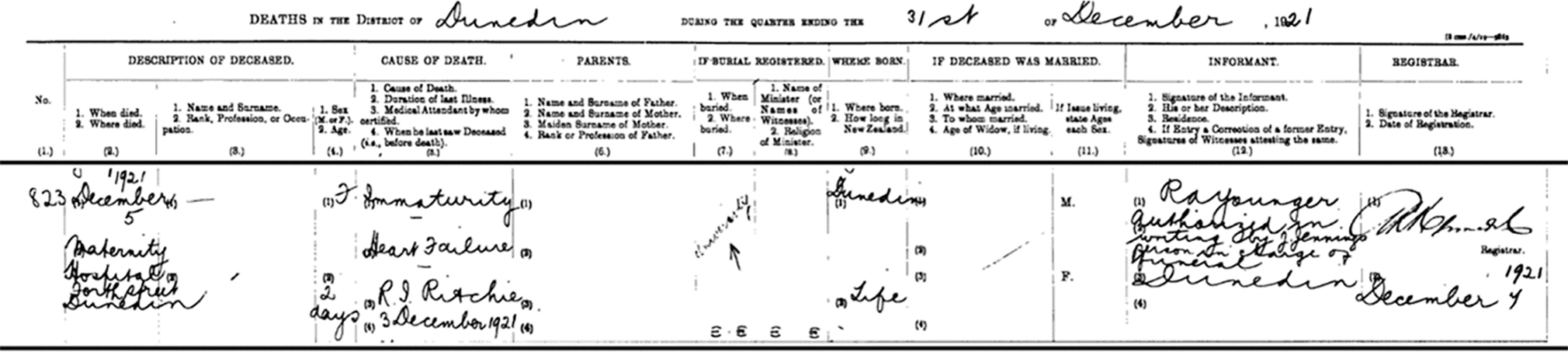
Figure 2. Example of a death certificate from the NZDIA. Name of the infant and their parent/s have been redacted.
Death certificates
Historical death certificates are held by the New Zealand Department of Internal Affairs. We investigated the death certificates of the infants noted in the University of Otago Register of Anatomical Material. The death certificates provide further detail in addition to the registers such as parental marital status, father’s occupation, burial location, and date of burial. They were used to provide information on the social status of the parent/s of these infants as well as confirm age-at-death and cause of death (see Figure 2 as an example).
Skeletal analysis
All fetal and infant remains were analyzed from the skeletal collection. The osteological analysis focused on estimating the minimum number of individuals (MNI) within the collection, estimating the age-at-death from each individual skeletal element (where possible), and macroscopic identification, description, and differential diagnosis of any pathology. No destructive analyses were undertaken on the remains.
MNI was important to estimate as most of the skeletal remains have been curated by skeletal elements (e.g., all loose infant and fetal frontal bones were curated together under one accession number), rather than by individual. There are some remains presented as complete individuals, either as articulated skeletons in anatomical position or laid out in glass cases, also in anatomical position. MNI can be calculated using the bone that is most frequently represented within the collection and the siding of these bones if they are paired. The most numerous bone within the infant and fetal skeletal remains of the W. D. Trotter Anatomy Museum collection was the squamous part of the occipital bone. As this is an unpaired bone, more than one in the collection represents more than one individual, regardless of age or sex.
An age estimation was obtained for each bone element where possible. All measurements of long bone length and cranial size were assessed using the standards from Fazekas and Kòsa (1978). Fazekas and Kòsa (1978) is the most complete standard available for age estimation of perinatal remains. Although other standards may be considered more methodologically sound due to being developed from individuals with a known age-at-death, Fazekas and Kòsa (1978) is the most widely accepted standard for estimating age from single skeletal elements (Cunningham et al. 2016; Lewis 2017; Michel and Charlier 2011; Pap and Pálfi 2011; Weidig et al. 2011). Poor maternal health and physiological stress can cause growth disruption and, in extreme cases, intrauterine growth restriction (IUGR), which may lead to underestimation of the age of these skeletal remains (Hendrix and Berghella 2008; Hoppa 2000; Merwin and Harris 1998; Perkins et. al. 2016). As growth disruption in fetal and infant skeletal remains is identified by comparing the age estimation from long bone length with age estimation from the dentition (Hodson and Gowland 2020), IUGR is unable to be conclusively diagnosed in this collection (or differentiated from younger fetuses who are a normal size) because the dental and remains are generally not curated together as individuals.
Age estimation based on dental development mitigates some of the limitations of skeletal aging methods as it is argued to be more tightly controlled by genetics and is therefore less susceptible to physiological stress (Bolaños et al. 2000; Liversidge and Molleson 2004; Thesleff 2000). For this research, estimating age from dental development is more appropriate than dental eruption methods as dental development methods can be used for perinatal individuals whose teeth have not yet erupted. Radiographs were taken to assess development of all dental remains. The standard used for this research was the London Atlas of Tooth Development and Eruption (AlQahtani et al. 2010; AlQahtani et al. 2014). Although this standard may not be considered the most accurate in estimating age from dental development in a modern New Zealand population (Baylis and Bassed 2017), the reference population of historic British and European juveniles reflects the predominantly European origin population of nineteenth-century Dunedin. The inclusion of fetal standards and clear differentiation of stages in perinatal development made the London Atlas of Tooth Development and Eruption the most suitable standard to use in this research. Sex estimation was not attempted as sexually dimorphic morphological characteristics are not sufficiently developed for conclusive sex estimation in preadolescent individuals (White and Folkens 2005).
Results
Analysis of the Register of Anatomical Materials showed 24 infants were acquired by the University of Otago from 1876–1941. Twenty perinates, one neonate, and three post-neonates were recorded as “supplied” to the university between 1876 and 1941 (Supplementary Table 1). There were six females, 12 males, and six individuals who did not have their sex recorded. The individuals are listed as year of death to protect their identity. Only four individuals from the Register of Anatomical Materials appeared in Gourley’s ledgers, also listed with the cost of “supplying” each individual to the university. Of the total number of infants, eight had prematurity or “immaturity” listed as cause of death. One who passed away from “prematurity” had a twin who survived (listed as “one breathes”). Two of the individuals died from trauma or birth complications, including hemorrhage. Two infants died of “inanition” and one of pyloric stenosis malnutrition. Six had congenital or birth defects, which may have made their bodies particularly interesting for use in anatomy education. Two died from infectious diseases: tuberculous enteritis and congenital syphilis. Two individuals had no cause of death listed.
Source of fetal and infant bodies
The infants supplied to the University of Otago from 1876 to 1941 were typically acquired from public institutions such as Batchelor Maternity Hospital (n = 11) and Dunedin Public Hospital (n = 9). Three individuals were supplied by the “Redroofs” Salvation Army Maternity home, one from Cook Maternity Home in Gisborne, and one individual from an unnamed maternity hospital (Supplementary Table 1). The most common source of infant bodies changes over time. Bodies predominately came from Dunedin Public Hospital in 1885–1920, whereas from 1921–1934, they were provided almost exclusively by Batchelor Hospital. Of the 24 infants in the University of Otago Register, there were 18 who had death records available. Seven of the 18 infants have father “not recorded” on the birth certificate, indicating they were “illegitimate” children to unmarried mothers (all those historical records with “illegitimate” were typed out with that information retracted). Those with a father recorded and their father’s profession recorded were mostly working class (e.g., laborers, bricklayers). Four have “university” noted in their “burial details” section in the death certificate (e.g., Fig. 2). Although many of the infants in the University Register note that they have been buried at various dates, with cross-referenced entries in Gourley’s registers reporting the location as Anderson Bay Cemetery, we find no evidence of burials of these individuals through the digitized burial records at the Anderson Bay Cemetery.
Although we have data on the acquisition of infants from the archival research, the skeletal remains in the museum are no longer linked to this information, and thus we cannot match the remains to any specific individual identity.
Osteological results
Based on the skeletal analysis, the minimum number of individuals within the fetal and infant collection is 32. The collection comprises different curation techniques (Table 2).
Most of the nonarticulated skeletal elements are from the cranium. Ribs, vertebrae, and pelvic bones were only found in the articulated or mounted individuals.
The general preservation of the skeletal tissue is excellent. The delicate skeletal elements of the crania, including the cranial vault bones and bones of the face, have been subject to some postmortem damage. Damage to the parietal bones is most common, as well as unilateral or bilateral damage to the zygomatic processes of the temporal bones.
Table 2. The Number of Articulated Skeletons, Articulated Crania or Skulls, and Nonarticulated Skeletal Elements in the W. D. Trotter Anatomy Museum
|
Curation Type |
Number |
|
Mounted or articulated skeleton, >90% complete |
6 |
|
Articulated cranium or skull |
13 |
|
Nonarticulated skeletal element |
267 |
Age-at-death
The age of the fetuses and infants ranges from 15 weeks gestation to 3 months postnatal (Fig. 3). Most of the skeletal elements are aged to be within the final month of pregnancy to full term (36–40 weeks gestation). Aging for individual skeletal elements is shown in Figure 4. Some individual skeletal elements (n = 51/296) were unable to be aged for one of three reasons: inability to access the element (some were encased in perspex or resin); postmortem damage to the element, making accurate measurement impossible (i.e., ethmoid); or lack of an aging standard for the skeletal element. These age estimations are presented below as both the age of the identified individuals within the collection (MNI = 32), as well as the age estimations for every individual skeletal element that was able to be analyzed. The skeletal element age distribution (Fig. 4) is included as it is more representative of the age distribution of the entire infant skeletal collection in the W. D. Trotter Anatomy Museum.
Pathology
Six of the 19 articulated individuals (five represented by articulated crania and one articulated skeleton) exhibited some form of visible skeletal pathology. Two of the five individuals represented by crania that exhibited pathology had trauma possibly related to delivery (O3.D15 and O3.D6), and four individuals exhibited pathology consistent with congenital developmental abnormalities (O3.D7, O3.D14, O3.D180, and O5.D1). One of these individuals with evidence for developmental pathology (O5.D1) is a complete articulated skeleton. Detailed descriptions of the pathological observations, photos, and differential diagnosis for each individual are included in Supplementary File 2.
Discussion
The main aim of this research was to provide an inventory of the fetal and infant skeletal remains of the W. D. Trotter Anatomy Museum and understand the social context in which these remains were acquired by the museum. To achieve this aim, the osteological evidence needs to be interpreted within the maternal and infant health context, in concert with archival data on their provenance and the social context of class, gender, and religion at the time that may have led to their acquisition and use in the museum context.
Although our data do not allow for us to identify the infant skeletal remains to any specific individual, the general age distribution as well as the causes of death and evidence of pathology on the bones of the fetuses and infants are similar between the skeletal remains and the available archival data. For example, we have two infants with skeletal evidence for cerebral trauma, and there are two infants who are noted in both their death certificates and University Register that they died from birth trauma. Similarly, we have evidence for individuals with developmental skeletal defects and many who are premature, and these etiologies are also documented in the historical archival research. We believe that the individuals may have been collected due to their pathologies and as examples of development (e.g., the premature infants). However, this is obviously a biased sample whereby infants who are born prematurely and those with developmental disorders are more likely to pass away.

Figure 3. Age-at-death distribution of the fetal and infant individuals of the W. D. Trotter Anatomy Museum collection. Those individuals older than 43 weeks gestational age are assumed to have been born alive and their death occurred within the neonatal or post-neonatal period.
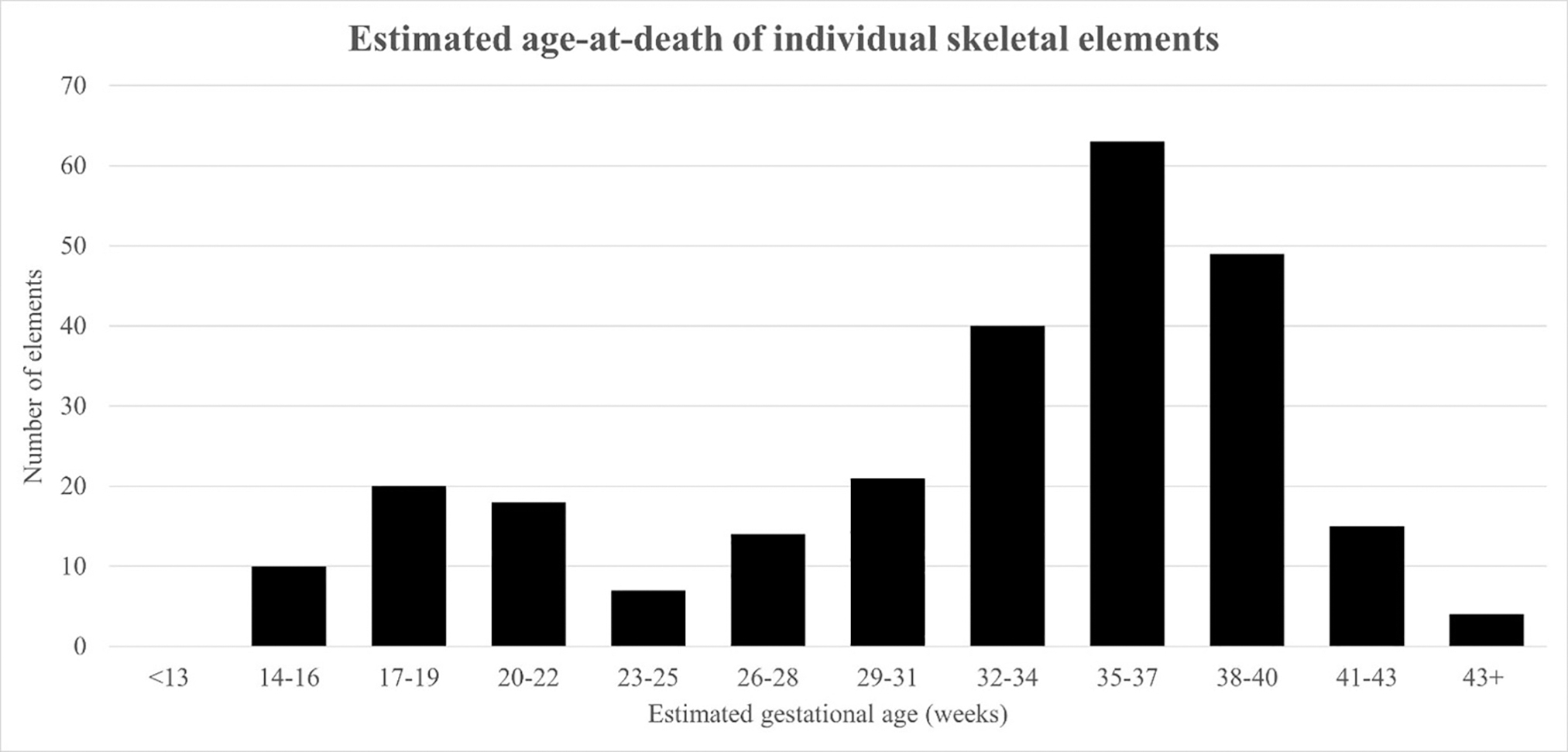
Figure 4. Age-at-death distribution for individual fetal and infant skeletal elements of the W. D. Trotter Anatomy Museum collection. Those individuals older than 43 weeks gestational age are assumed to have been born alive and their death occurred within the neonatal or post-neonatal period.
Infant and maternal mortality in New Zealand
Assessing the osteological evidence of age-at-death and pathology, using knowledge of historical causes of fetal and infant death in New Zealand is important in considering the possible causes of death for these infants in the W. D. Trotter Museum. Common causes of maternal death are important to explore also, as maternal and fetal health are inextricably linked (Lassi et al. 2013) and infants who lost their mother at birth tended to have poorer health outcomes (Atrash 2011; Clarke 2012; Loudon 1991; Pavard et al. 2005; Sadetskaya and Oxley 2012).
In New Zealand, infant mortality peaked in 1875 at 130 deaths per 1,000 live births and then began to decline thereafter (Fraser 1928), similarly to other developed countries at this time (Loudon 1991; Sadetskaya 2015; Sadetskaya and Oxley 2012). By 1920, this mortality rate had more than halved due to the improvements in maternal and infant care. It is argued, however, that this decline in infant mortality was only experienced by the Pākehā (white New Zealander) population (Pool et al. 2007; Sadetskaya 2015), with the Māori mortality rates excluded in published data until 1920 (Sheehan 1878; Waldegrave 1901; Ward 1905). Once introduced, Māori registration data continued to be of poor quality (Pool 1973), and therefore the true Māori infant mortality rate during the nineteenth and early twentieth centuries remains unknown, with modern estimations placing it much higher than the Pākehā recorded infant mortality rate (Statistics New Zealand 2006). Despite improvements in public health and medical treatment during the early twentieth century, the major causes of infant death have not changed significantly since the nineteenth century, with the main causes being prematurity and respiratory and diarrheal diseases (Clarke 2012; Fraser 1928; Loudon 1991). There was no formal requirement to register stillbirth in New Zealand until 1919, but some earlier parents chose to register their stillborn child. Poor obstetric technique contributed to both infant and maternal mortality, with some of the methods developed for dealing with maternal health conditions such as eclampsia causing trauma for both mother and child (Bryder 1986; Drife 2002; Loudon 1986; Sheikh et al. 2013). The use of accouchement forcé, high forceps early in labor, and nonsterile techniques posed significant risk to both mother and child and were at times used without clinical need (Bryder 1986; Drife 2002; Loudon 1986; Sheikh et al. 2013). This risk is seen in the individuals who have evidence for forceps trauma from the skeletal evidence.
Societal reactions to infant and fetal loss
Assessing prenatal loss is especially important because the societal response to an individual who died before birth may have impacted the decisions made by parents after death regarding burial or donation of the remains of their baby, including dissection or donation to a museum. The infants in the W. D. Trotter Anatomy Museum were not treated in the normative way in terms of religious and spiritual needs of burial on consecrated ground. This indicates that despite going against social norms, it was seen as imperative (by the medical community at least) for these bodies to be used in teaching and research context at the time and that their educational value overrode the need for normative burial.
Most of the infants in the collection are aged around full term (40 weeks) or younger. Defining stillbirth in a historic osteological context is difficult; in this research, any individual with an estimated age-at-death between 20 and 40 weeks gestation is considered a possible stillbirth. The role of religion in society can impact on the choices available for burial of stillborn children (Murphy 2011). In some religions, receiving God’s forgiveness before death (through baptism or other penitential rites) was a way to ease the road of the departed to Heaven (Murphy 2011). Baptism was also often a criterion for burial in a religious burial ground but could only be performed on live children (Cootes 2021; Murphy 2011; Perry 1983). If a child looked to be in distress after birth, emergency baptism could be performed by a layperson to ensure the safe passage of their soul to Heaven (Code of Canon Law 1983; Clarke 2012). Under the Cemeteries Bill (New Zealand) 1880, the consecrated areas of cemeteries were exclusively under the authority of the church that consecrated them. This meant that children who were not baptized may not have been able to be buried in consecrated ground, depending on the doctrine of the controlling church (Murphy 2011). This could be a source of pain for a deeply religious family and potentially impact the decisions they would make regarding the care of their child after death. While the burial of stillborn children in consecrated ground may have been prevented, public cemeteries and some denominations did allow for the burial of stillborn children (Ockwell 1978, 1982), as was the case in Dunedin. Archaeological evidence from Canada and the United Kingdom also indicates that burial of stillborns was not uncommon (Davis 2009; Herring et al. 1991). In New Zealand, there was no framework for registering stillbirths until 1913 and no requirement to register stillbirths until 1919 (Birth and Deaths Registration Amendment Act 1912); consequently, nineteenth-century stillbirth rates are unknown. Experienced New Zealand physicians Ernest Rawson and William Sealy estimated that stillbirths made up 3% to 5% of the births they attended between 1859 and 1895 (Clarke 2012).
Infant loss and family grief
She has no Baby now to call her Mother. (Eliza White diary 1830, cited in Clarke 2012:223)
To understand the significance of the accession of the infants in the museum, a consideration of emotional responses to infant death and normative funerary ritual is important. Since the 1960s, some anthropological and archaeological literature has suggested that in times of high infant mortality, parents would restrain themselves from emotionally investing in their infants to prevent overwhelming grief if the child was to die and can be used to explain infant atypical burial (Ariès 1962; Cannon and Cook 2015; Jalland 1996; Parkes 1986; Pollock 1983; Stone 1977). The theory of withholding of grief does not fit with evidence for attitudes toward infant loss in historic New Zealand. Unfortunately, the relatively high infant mortality rates of the late nineteenth century meant that the reality of infant death was something many families faced (Clarke 2012; Jalland 1996). During Victorian and Edwardian times, there are obvious signs of public displays of grief, which can be contrasted to today’s stigma and silence surrounding pregnancy loss or the loss of an infant (Gowland 2020). For instance, there are primary accounts from New Zealand that show that miscarriage, stillbirth, and the death of a child were all discussed in personal letters between friends and family and even announced in the newspapers (Clarke 2012; Clutha Leader 1894; Mount Ida Chronicle 1881; Porter and MacDonald 1996) (e.g., Fig. 5).
Pākehā funerary practices in nineteenth-century New Zealand followed those of Victorian England and were involved and elaborate (Bedikian 2008; Schafer 2007). Family involvement with the body of the deceased was common in the United Kingdom, with relatives often congregating in one room with the body for several days (Murdoch 2015). Postmortem photography and large funeral processions would precede interment within the week after death (Murdoch 2015). Children’s deaths were seen as particularly tragic for the family (Jalland 1996) and were mourned accordingly, with the same funerary practices and interment rights afforded to children as to adults. One exception to this may have been interment rights for stillborn children, who were possibly restricted from burial in denominational areas of cemeteries, as discussed previously.
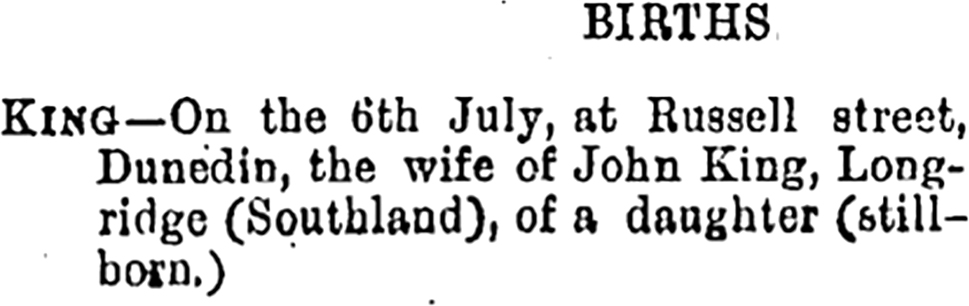
Figure 5. An example of an announcement of stillbirth; Mataura Ensign, 12 July 1887. Courtesy of The National Library of New Zealand | Te Puna Mātauranga o Aotearoa.
Although it is highly unlikely the infant and fetal remains of the W. D. Trotter Anatomy Museum are of Māori ancestry, discussion of infant death and mortuary treatment within Māori culture is relevant, even if to rule out this possibility. In Māori culture, the correct treatment of a stillborn child after death was imperative, as the souls of stillborn children were believed to become malignant spirits (kehua) after death. Kehua could cause severe illness among members of the iwi (tribe) and so the burial rites were particularly important to ensure the passage of the soul to Rangi (heaven) or Te Po (the underworld) and prevent the soul staying on earth, where it could cause harm (Goldie 1904). The community would come together at the marae (meeting house) for days of whaikōrero (speeches), waiata (songs), karakia (prayer), poroporoaki (speeches of farewell), and tangi (mourning) (Jacob et al. 2011). The entire community (including children) would take part in this process, and burial would only occur after all the marae rituals were completed (Jacob et al. 2011).
Acquisition of human remains for education in New Zealand
In many modern “Western” cultures, an individual is often imbued with personhood throughout gestation, and identity acquisition begins in the womb (Gowland 2020; Gowland et al. 2014). This concept of personhood in infants is enshrined in New Zealand legislation that governs modern collections such as the W. D. Trotter Anatomy Museum. Since 2008, in New Zealand, fetal and infant tissue has been unable to be acquired (Human Tissue Act 2008, section 8(b)). If modern legislation effectively bans the collection of fetal and infant tissue under the guise of the individual being unable to consent, why was the acquisition, preservation, and storage of infant and fetal tissue considered appropriate in nineteenth-century New Zealand? This can be understood within the different social context from when the remains were acquired. The fetal and infant skeletal remains were collected when the Anatomy Act 1875 was the governing legislation for schools of anatomy. This act, modeled on the 1832 UK Anatomy Act, allowed for the dissection of human remains by the schools of anatomy if permission for dissection was given by the individual with legal custody of the body after death (Anatomy Act 1875). This law theoretically allowed for any individual to undergo dissection, including women and children, unless they had explicitly stated they did not want to undergo dissection (Anatomy Act 1875). In line with evidence from skeletal collections from other parts of the world, it is likely these remains were collected to study development and pathology (Dittmar and Mitchell 2016), and the continued preferential holding of these remains over (anatomically normal) males dissected over the past 150 years at the Otago Medical School suggests they were valued for their rarity and role in education.
The purchase of skeletal remains was a fast and straightforward way to build a collection from the mid-nineteenth to late twentieth centuries during the formative period for anatomization of human material (Hefner et al. 2016). India was the primary source of (adult) skeletal remains, which were unfortunately often robbed from graves, coerced from families, or taken under false pretenses such as for postmortem examinations and then processed for medical use (Hefner et al. 2016). However, acquisition records indicate the primary sources of infant remains for the Medical School include being donated or acquired from the local community immediately after their deaths. It may be that the infants that were acquired for cadaveric dissection remain in the W. D. Trotter Anatomy Museum today. Of the four individuals also found in Gourley’s ledgers, three were listed as having a cost for the “University” as a part of the entry, for “supplying” the body. The typical cost for supplying a body to the institution was £5 (which translates to roughly $1,151 NZD in 2023), but the cost associated with one infant, who died in Dunedin from a cerebral hemorrhage, cost £31, which amounts to a modern $7,137 NZD. The willingness to pay the relatively high cost associated with obtaining these remains for anatomy education suggests the high demand for cadavers in Dunedin. There is no evidence from any historical sources for widespread graverobbing of bodies for use in anatomical education within the New Zealand context.
Body donation of infants, medical authority, and the intersection of class, stigma, and structural violence
Body donation in nineteenth-century New Zealand was almost unrecognizable from the modern body bequest program in place at the University of Otago. The current body bequest program at the University of Otago, in line with the New Zealand Human Tissue Act 2008, requires informed, clear, written consent from the individual and the individual’s family. One of the desired outcomes of the Anatomy Act 1875 was to increase the availability of cadavers for medical education (Jones and Whitaker 2012). This was to prevent graverobbing, which had been a major problem in the United Kingdom (Dittmar and Mitchell 2016; Jones and Whitaker 2012). The supply of cadavers for education was increased by the law allowing the use of unclaimed bodies for dissection (Anatomy Act 1875). Once again, this law disproportionately affected the poor and mentally ill (Jones and Whitaker 2012). Those who had sought help during their lifetime (including poor pregnant women) and died while in care were now available for dissection at the discretion of the warden or surgeon, who were afforded a large amount of authority in this context.
Our historical analysis focusing on the accession registers and sources of bodies proves that this was indeed the case. Dunedin Public Hospital, the Otago Benevolent Institution, “Redroofs” Salvation Army House, the Batchelor Maternity Hospital, and Cook Maternity Home in Gisborne were the places of death on the records for these infants. These hospitals provided care beyond the immediate pre- and postnatal period for poor women and their children (Clarke 2012). “Redroofs,” alongside other Salvation Army Houses across the country, specifically aided single or unwed mothers for a brief period before and after birth. The marital status and socio-economic status information that we have for these mothers is discussed below.
The Anatomy Act 1875 required consent only from the person who had legal custody of the body after death unless the prospective donor had objected to dissection either verbally or in writing during their lifetime. In most situations, the family would have legal custody of an individual’s body after death and therefore familial consent would be required for the donation of the body to the university. If an individual died in hospital, prison, or an asylum, the surgeon or warden in charge of the institution had legal custody of the body. The University of Otago sought out these bodies; the first cadaver dissected at the University of Otago was that of a man who had died in Dunedin Public Hospital (Carmalt Jones 1945). Dunedin Public Hospital and the University of Otago were closely linked; many of the lecturers at the medical school also worked in the hospital (Carmalt Jones 1945; Hercus and Bell 1964), and it remains a teaching hospital to this day. It is likely that many of the remains of the fetal and infant individuals within the collection were donated by the hospital physicians because the records show that all the infants accessioned listed in the Register of Anatomical Material died while in a hospital.
In this case, the Anatomy Act 1875 disproportionately affected poor families. In nineteenth-century New Zealand, hospital birth was seen as a last resort. Many towns refused to open a maternity ward at all, believing they were vectors for infection (Clarke 2012). Middle-class and wealthy women gave birth at home, attended by midwives or a doctor (Clarke 2012), in which case, the family would maintain legal custody of the child should it pass away or be stillborn. The majority of women giving birth in hospitals in the nineteenth century were poor or without familial support; therefore, the legal chain of custody meant that poor women were the most likely to be left without a choice in regard to the resting place of their children if they were stillborn or died soon after birth, which may have led to the acquisition of their infants for use in the Medical School and museum context. The presence of individuals with developmental anomalies within the collection also suggests that hospital care may have been required for these individuals in their short life and they may have died in hospital. Some may also have been selectively curated within the collection as examples of pathology, a way to demonstrate abnormalities in development to medical students.
No further record of burial could be identified for any of the infants detailed in the Register of Anatomical Material. While the register denotes a date of burial (for some, but not all the infants), there are no Dunedin City Council records of burial for these infants. If in fact these infants were not buried, this is a major indication that they were treated differently in death than many of the adult cadavers who were buried. The collection and anatomization of fetuses was highly valued in the advancement of scientific careers and social prestige (Franzén 2022; Wilkie 2003), where curators and anatomists went through a phase of amassing “material” in the nineteenth century (Teather 1990). In the nineteenth- and twentieth-century United States, women were given little to no agency in this process of the acquisition of their infants in the anatomical context, and most were not aware that their baby had been taken away (Dubow 2011; Noe 2004. Morgan (2002, 2004, 2009) has explored from a medical anthropological point of view the place anatomical collectors and preparers play in the transformation of embryos and fetuses in the social context of turning something that is mostly socially unrecognizable (e.g., early pregnancy) into an object of cultural and social importance (Morgan 2009:5). Franzén (2022) found in the context of acquisition of fetal bodies by Uppsala University from ca. 1890–1930 that mothers had different understandings of fetal bodies and notions of their care than the physicians and anatomists.
Although the infant and fetal remains in the W. D. Trotter Anatomy Museum may have been donated by the surgeon of the hospital they died in, it is also possible that some of the families may have chosen to donate the bodies of their children to support medical education or for other unspecified reasons, but this is unknown. The individual reasons behind body donation are varied and complex, and parents may have chosen body donation or to leave the remains of their child unclaimed for social, religious, or more pragmatic reasons (Fennell and Jones 1992).
Structural violence toward women was a factor contributing to the acquisition of infant bodies for education. As stated, structural violence is harm perpetuated against individuals or groups through the normalization of inequalities embedded within social structures and institutions (Galtung 1969; Rylko-Bauer and Farmer 2016), and this can be extended to the acquisition of human remains and dissection of these remains in anatomy (Nystrom 2014). A significant proportion of the infants who were used in the W. D. Trotter Anatomy Museum were born to unmarried mothers, and those who were married were mostly from low-class families, as evidenced by the occupations of their husbands. There were many mechanisms through which structural violence impacted women. The patriarchal society of colonial New Zealand placed blame for rape and coercive sexual encounters on women (NZ Truth 1908). Social stigma surrounding pregnancy out of wedlock painted women as “shiftless and immoral” or “sinners” (Garlick 2012; NZ Truth 1908) and forced women out of jobs, therefore making them reliant on social institutions (such as parishes and Benevolent Institutions, which often had discriminatory policies toward pregnant women) or family for material assistance (Clarke 2012; Destitute Persons Act 1846; Garlick 2012; Hospital and Charitable Institutions Act 1885). Poor pregnant women, if not already institutionalized, were forced to give birth without medical care or attend hospital (O’Donnell 1991). Mothers with financial means in nineteenth- and early twentieth-century New Zealand would typically avoid giving birth in public hospitals, instead seeking maternity care in their own home from a private doctor, midwife, or nurse (Clarke 2012). Some mothers had no choice but to give birth in the public hospital, either due to financial constraints or perceived social deviance (i.e., being a single mother) (O’Donnell 1991). Hospital births could violate women’s autonomy, leaving them alone at the hands of male doctors, with no choice in their own birth experience, and legally no custody of the body of their child should they die in hospital (the mother’s body would also remain in the custody of the surgeon, should she die while admitted) (Anatomy Act 1875). The social circumstances of a woman affected the health care she was able to access, the care she was entitled to, and the choices she was able to make for her own body and the body of her child.
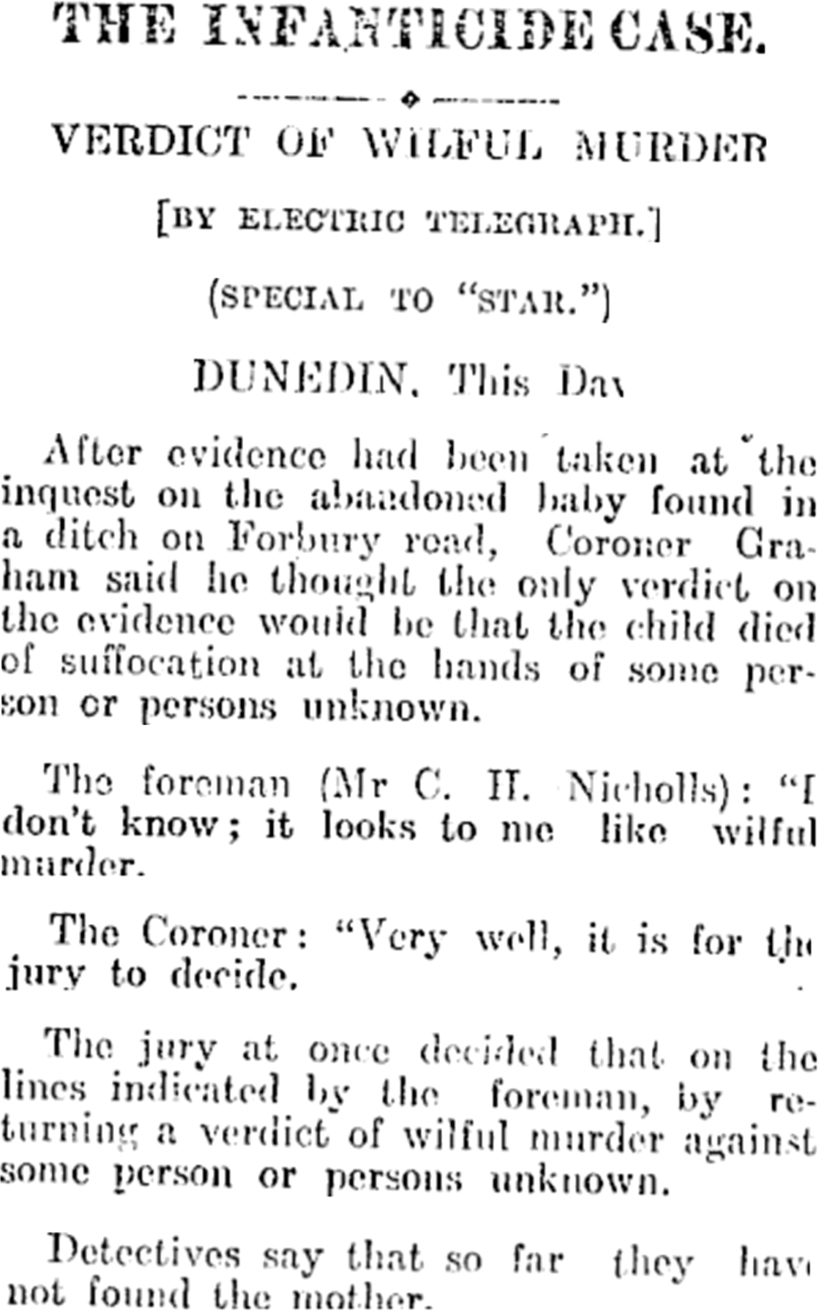
Figure 6. Newspaper article on verdict of infanticide by abandonment, with mother unknown. Source: Greymouth Evening Star, 18 June 1904, p. 4.
There is evidence for the abandonment of infants and infanticide at the end of the nineteenth century and early twentieth century in Dunedin, with many of these infants remaining unidentified (e.g., Fig. 6). Clarke (2012) reviewed several cases, many of whom were from Dunedin, which was the biggest center in New Zealand at the time. These infants would have been likely candidates for medical dissection and curation in the museum. Many of the infants who were identified in these circumstances were “illegitimate” (Clarke 2012) and therefore victims of structural violence through lack of social support for women within a patriarchal society where being an unmarried mother meant you could be shamed and unsupported at various levels in society.
Conclusion
Little research has focused on the fetal and infant remains of anatomy museums around the globe (Dittmar and Mitchell 2016; Muller and Butler 2018). In the museum and education environment, bodies have, especially in the past, been objectified as anatomical specimens rather than the individuals these remains belong to, nor has the social context been assessed that culminated in their curation in these institutions’ collections. Fetal and infant remains from historical anatomical collections can provide important insight into the lives of mothers and infants during the time the remains were acquired and their social context. The osteological analyses found that there is a range of bones from individuals of different ages and the presence of developmental pathology, emphasizing their value as developmental resources at the time of acquisition and the authority afforded to the physicians in collecting them. Most individuals were aged at around full-term, mimicking the normal age-at-death distribution of infants. There is osteological evidence for two individuals dying around the time of death from birth trauma, one including the possible use of forceps during birth, and there is evidence for dissection on some individuals. There is also osteological evidence for four individuals with skeletal developmental anomalies whose skeletal remains may have been kept for dissection and education as examples of anatomical “oddities.” The archival evidence on age-at-death and cause of death is similar to the osteological evidence. However, because of the loss of provenience information for individuals still housed in the collection, we are unable to identify the human remains to specific individuals. The archival evidence and social historical context give us insight into their acquisition through the consideration of structural violence at the nexus of factors including class and social stigma of unwed pregnant people, affecting the treatment of parents and the treatment of their deceased infants, with marginalization in death as they had during their short life. These factors should be addressed in the retention of these remains and in their use in education and research.
Ethics Statement
We approached the University of Otago Ethics Committee and the New Zealand Department of Internal Affairs | Te Tari Taiwhenua for our archival research using the publicly available ledgers and death certificates and were advised that no ethical review was required so long as our data collection and publications of this information comply with all relevant legislation (i.e., Privacy Act 2020, Births, Deaths, Marriages and Relationships Registration Act 2021, Health Information Privacy Code 2020, Human Tissue Act 2008, etc.). Permission from the Hocken Library | Uare Taoka o Hākena was obtained for the use of Figure 1. Ethics approval for the osteological research was gained from the University of Otago Department of Anatomy Body Ethics Committee.
Acknowledgments
Thank you to Gillions Funeral Services Ltd. for access to the archives and to the Hocken Librarians for their help with access to the collection and their copying of Figure 1. Part of the archival work was funded by the Department of Anatomy Summer Scholarship from the University of Otago awarded to ES and funding from the Performance Based Research Fund awarded to SH. We also thank Annella MacArthur, Sara Otto and Stephie Lončar for their language expertise in translating the abstract. We are especially grateful to Annella MacArthur for her expertise in translating the abstract into Scottish Gaelic, a language with a rich cultural heritage that remains a vital part of our history. We thank the Associate Editor, Co-Editor-in-Chief (Gwen Robbins Schug), and reviewers for their constructive comments challenging us to reflect on how to appropriately present these infants housed within the W. D. Trotter Museum, which is not an easy story to tell.
References Cited
Adams, M. 2009. Both sides of the collecting encounter: The George W. Harley collection at the Peabody Museum of archaeology and ethnology, Harvard University. Museum Anthropology 32(1): 17–32. DOI: 10.1111/j.1548-1379.2009.01018.x.
Aleck, K. 2004. Craniosynostosis syndromes in the genomic era. Seminars in Pediatric Neurology 11(4):256–261. DOI: 10.1016/j.spen.2004.10.005.
Alberti, S. 2011. Medical museums past, present and future. The Bulletin of the Royal College of Surgeons of England 93(2):56–58. DOI: 10.1308/147363511X552548.
Al-Namnam, N. M., F. Hariri, M. K. Thong, and Z. A. Rahman. 2019. Crouzon syndrome: Genetic and intervention review. Journal of Oral Biology and Craniofacial Research 9:37–39. DOI: 10.1016/j.jobcr.2018.08.007.
AlQahtani, S. J., M. P. Hector, and H. M. Liversidge. 2014. Accuracy of dental age estimation charts: Schour and Massler, Ubelaker and the London Atlas. American Journal of Physical Anthropology 154(1):70–78. DOI: 10.1002/ajpa.22473.
AlQahtani, S. J., M. P. Hector, and H. M. Liversidge. 2010. Brief communication: The London Atlas of Human Tooth Development and Eruption. American Journal of Physical Anthropology 142(3):481–490. DOI: 10.1002/ajpa.21258.
Ami, O., J. C. Maran, P. Gabor, E. B. Whitacre, D. Musset, C. Dubray, et al. 2019. Three-dimensional magnetic resonance imaging of fetal head molding and brain shape changes during the second stage of labor. PLoS ONE 14(5):e0215721 DOI: 10.1371/JOURNAL.PONE.0215721.
“An act for regulating schools of anatomy 1832.” (Anatomy Act 1832 (GB)). http://www.irishstatutebook.ie/eli/1832/act/75/enacted/en/print.html
Anatomy Act. 1875. New Zealand. http://www.nzlii.org/nz/legis/hist_act/aa187539v1875n42223/. Accessed 10 December 2021.
Ariès, P. 1962. Centuries of Childhood. Cape, London.
Atrash, H. K. 2011. Parents’ death and its implications for child survival. Revista brasileira de crescimento e desenvolvimento humano 21(3):759–770.
Aufderheide, A. C., and C. Rodríguez-Martin. 1998. The Cambridge Encyclopedia of Human Paleopathology. Cambridge University Press, Cambridge.
Aumüller, G., and C. Lenk. 2022. The Marburg Museum Anatomicum and its unusual gynecological specimens: A brief history and ethical contextualisation. Annals of Anatomy—Anatomischer Anzeiger 244:151989. DOI: 10.1016/J.AANAT.2022.151989.
Barden, H. S. 1983. Growth and development of selected hard tissues in Down syndrome: A review. Human Biology 55(3):539–576.
Baylis, S., and R. Bassed. 2017. Precision and accuracy of commonly used dental age estimation charts for the New Zealand population. Forensic Science International 277:223–228. DOI: 10.1016/j.forsciint.2017.06.011.
Bedikian, S. A. 2008. The death of mourning: From Victorian crepe to the little black dress. Omega: Journal of Death and Dying 57(1):35–52. DOI: 10.2190/OM.57.1.c.
Beiter, K. J., S. E. Fourniquet, and J. C. Mussell. 2019. Incorporating fetal archival tissues into undergraduate medical education. The FASEB Journal 33(Suppl. 1):607.3. DOI: 10.1096/FASEBJ.2019.33.1_SUPPLEMENT.607.3.
Benjamin, I., R. Johns, O. Oseji, T. Anderson, F. Mercardo, V. Arruana, et al. 2022. Polydactyly of the fetal foot: A case report and review of the literature. Journal of the National Medical Association 114(4):406–411. DOI: 10.1016/j.jnma.2022.03.001.
Bernstein, I. M., J. D. Horbar, G. J. Badger, A. Ohlsson, and A. Golan. 2000. Morbidity and mortality among very-low-birth-weight neonates with intrauterine growth restriction. American Journal of Obstetrics and Gynecology 182(1):198–206. DOI: 10.1016/S0002-9378(00)70513-8.
Biers, T. 2020. Rethinking purpose, protocol, and popularity in displaying the dead in museums. In Ethical Approaches to Human Remains: A Global Challenge in Bioarchaeology and Forensic Anthropology, edited by K. Squires, D. Errickson, and N. Márquez-Grant. Springer, Cham, pp. 239–263. https://doi.org/10.1007/978-3-030-32926-6_11/COVER
Birth Announcements. 1894. Mount Ida Chronicle, May 5. https://paperspast.natlib.govt.nz/newspapers/MIC18810505.2.5. Accessed 10 December 2021.
Birth Announcements. 1894. Clutha Leader, March 9. https://paperspast.natlib.govt.nz/newspapers/CL18940309.2.9. Accessed 10 December 2021.
Births and Deaths Registration Amendment Act 1912 (New Zealand). http://www.nzlii.org/nz/legis/hist_act/badraa19123gv1912n18453/. Accessed 19 July 2021.
Bolaños, M. V., M. C. Manrique, M. J. Bolaños, and M. T. Briones. 2000. Approaches to chronological age assessment based on dental calcification. Forensic Science International 110(2):97–106. DOI: 10.1016/S0379-0738(00)00154-7.
Bonney, H., J. Bekvalac, and C. Phillips. 2020. Human remains in museum collections in the United Kingdom. In Ethical Approaches to Human Remains: A Global Challenge in Bioarchaeology and Forensic Anthropology, edited by K. Squires, D. Errickson, and N. Márquez-Grant. Springer, Cham, pp. 211–237. DOI: 10.1007/978-3-030-32926-6_10/COVER.
Brickley, M., and R. Ives. 2008. Vitamin D deficiency. In The Bioarchaeology of Metabolic Bone Disease, edited by M. Brinkley and R. Ives. Academic Press, London, pp. 75–150. DOI: 10.1016/B978-0-12-370486-3.50018-3.
Bring, H. S., I. A. Hulthén Varli, M. Kublickas, N. Papadogiannakis, and K. Pettersson. 2014. Causes of stillbirth at different gestational ages in singleton pregnancies. Acta Obstetricia et Gynecologica Scandinavica 93(1):86–92. DOI: 10.1111/aogs.12278
Bryder, L. 1986. Maternity in Dispute: New Zealand 1920-1939. Historical Publications Branch, Department of Internal Affairs, Wellington.
Buchmann, E. J., and E. Libhaber. 2008. Sagittal suture overlap in cephalopelvic disproportion: Blinded and non-participant assessment. Acta Obstetricia et Gynecologica Scandinavica 87(7):731–737. DOI: 10.1080/00016340802179848.
Cannon, A., and K. Cook. 2015. Infant death and the archaeology of grief. Cambridge Archaeological Journal 25(2):399–416. DOI: 10.1017/S0959774315000049.
Carey, J. C. 2021. Trisomy 18 and trisomy 13 syndromes. In Cassidy and Allanson’s Management of Genetic Syndromes, edited by John C. Carey, Agatino Battaglia, David Viskochil, and Suzanne B. Cassidy. John Wiley and Sons, Hoboken, NJ, pp. 937–956.
Carmalt Jones, D. W. 1945. Annals of the University of Otago Medical School. A. H. & A. W. Reed, Wellington.
Cereda, A., and J. C. Carey. 2012. The trisomy 18 syndrome. Orphanet Journal of Rare Diseases 7:81. DOI: 10.1186/1750-1172-7-81.
Chasler, C. N. 1967. The newborn skull: The diagnosis of fracture. American Journal of Roentgenology 100(1):92–99.
Claes, T., and V. Deblon. 2018. When nothing remains: Anatomical collections, the ethics of stewardship and the meanings of absence. Journal of the History of Collections 30(2):351–362. DOI: 10.1093/JHC/FHX019.
Clarke, A. 2012. Born to a Changing World: Childbirth in Nineteenth-Century New Zealand. Bridget Williams Books, Wellington.
The Code of Canon Law. 1983. Canon 867. https://www.vatican.va/archive/cod-iuris-canonici/eng/documents/cic_lib4-cann834-878_en.html#CHAPTER_III. Accessed 10 December 2021.
Comer, A. R. 2022. The evolving ethics of anatomy: Dissecting an unethical past in order to prepare for a future of ethical anatomical practice. The Anatomical Record 305(4):818–826. DOI: 10.1002/AR.24868.
Cox, D. R. 2019. The ancient taboo of miscarriage. InnovAiT 13(1):61–62. DOI: 10.1177/1755738019828200.
Cunningham, C., L. Scheuer, and S. Black. 2016. Developmental Juvenile Osteology. 2nd ed. Elsevier, London.
Davis, G. 2009. Stillbirth registration and perceptions of infant death, 1900-60: The Scottish case in national context. Economic History Review 62(3):629–654. DOI: 10.1111/j.1468-0289.2009.00478.x.
de la Cova, C. 2011. Race, health, and disease in 19th-century-born males. American Journal of Physical Anthropology 144(4):526–537. https://doi.org/10.1002/ajpa.21434.
de la Cova, C. 2019. Marginalized bodies and the construction of the Robert J. Terry anatomical skeletal collection: A promised land lost. In Bioarchaeology of Marginalized People, edited by M. L. Mant and A. Jaagumägi Holland. Academic Press, London, pp. 133–155. DOI: 10.1016/B978-0-12-815224-9.00007-5
DeLee, J. B. 1920. The prophylactic forceps operation. American Journal of Obstetrics and Gynecology 1(1):34–44. DOI: 10.1016/s0002-9378(20)90067-4
Destitute Persons Act. 1846. http://www.nzlii.org/nz/legis/hist_act/dpa184610v1846n9354/. Accessed 10 December 2021.
Dine, R. L. 2019. You shall bury him: Burial, suicide and the development of Catholic law and theology. Medical Humanities 46:299–310. DOI: 10.1136/medhum-2018-011622
Dittmar, J. M., and P. D. Mitchell. 2016. From cradle to grave via the dissection room: The role of foetal and infant bodies in anatomical education from the late 1700s to early 1900s. Journal of Anatomy 229(6):713–722.
Dittmar, J. M., and P. D. Mitchell. 2018. Equality after death: Dissection of the female body in anatomical education during the 19th century. Bioarchaeology International 2(4):283–293. DOI: 10.5744/bi.2019.1002.
Dolea, C., and C. AbouZahr. 2000. Global Burden of Obstructed Labour in the Year 2000. World Health Organization, Geneva.
Drife, J. 2002. The start of life: A history of obstetrics. Postgraduate Medical Journal 78:311–315. DOI: 10.1136/pmj.78.919.311.
Dubow, S. 2011. Ourselves Unborn: A History of the Fetus in Modern America. Oxford University Press, Oxford.
Dupuis, O., R. Silveira, C. Dupont, C. Mottolese, P. Kahn, A. Dittmar, et al. 2005. Comparison of “instrument-associated” and “spontaneous” obstetric depressed skull fractures in a cohort of 68 neonates. American Journal of Obstetrics and Gynecology 192(1):165–170. DOI: 10.1016/j.ajog.2004.06.035
Fazekas, I. G., and F. Kósa. 1978. Forensic Fetal Osteology. Akadémiai Kiadó, Budapest.
Fennell, S., and D. G. Jones. 1992. The bequest of human bodies for dissection: A case study in the Otago Medical School. New Zealand Medical Journal 105:472–474.
Fourniquet, S. E., K. J. Beiter, and J. C. Mussell. 2019. Ethical rationales and guidelines for the continued use of archival collections of embryonic and fetal specimens. Anatomical Sciences Education 12(4):407–416. DOI: 10.1002/ASE.1897.
Franzén, H. 2022. "The precious material": Obtaining human fetal bodies for an embryological collection at Uppsala University, ca 1890-1930. Scandinavian Journal of History 47(2): 178–202. DOI: 10.1080/03468755.2021.1985602
Fraser, M. 1928. New Zealand: Infant mortality rates and still births. Economic Record 4:27–28.
Galtung, J. 1969. Violence, peace, and peace research. Journal of Peace Research 6(3):167–191.
Garlick, T. 2012. Social Developments: An Organisational History of the Ministry of Social Development and Its Predecessors, 1860-2011. Steele Roberts, Wellington.
Giancotti, A., V. D’Ambrosio, E. Marchionni, A. Squarcella, C. Aliberti, R. La Torre, et al. 2017. Pfeiffer syndrome: Literature review of prenatal sonographic findings and genetic diagnosis. Journal of Maternal-Fetal and Neonatal Medicine 30:2225–2231. DOI: 10.1080/14767058.2016.1243099.
Goldie, W. H. 1904. Māori medical lore: Notes on the causes of disease and treatment of the sick among the Māori people of New Zealand; as believed and practised in former times, together with some account of various ancient rites connected with the same. Transactions and Proceedings of the Royal Society of New Zealand 37:1–120.
Governale, L. S. 2015. Craniosynostosis. Pediatric Neurology 53(5):394–401. DOI: https://doi.org/10.1016/j.pediatrneurol.2015.07.006.
Gowland, R. L. 2020. Ruptured: Reproductive loss, bodily boundaries, time and the life course in archaeology. In The Mother-Infant Nexus in Anthropology: Small Beginnings, Significant Outcomes, edited by R. Gowland and S. E. Halcrow. Springer Nature, Cham, pp. 257–274.
Gowland, R. L., A. T. Chamberlain, and R. C. Redfern. 2014. On the brink of being: Re-evaluating infanticide and infant burial in Roman Britain. Journal of Roman Archaeology Supplementary Series 96:69–88.
Gowland, R. L., and S. E. Halcrow, eds. 2020. The Mother-Infant Nexus in Anthropology: Small Beginnings, Significant Outcomes. Springer Nature, Cham.
Halcrow, S. E., and N. Tayles. 2008. The bioarchaeological investigation of childhood and social age: Problems and prospects. Journal of Archaeological Method and Theory 15(2):190–215. DOI: 10.1007/s10816-008-9052-x.
Halcrow, S. E., N. Tayles, and G. E. Elliott. 2017. The bioarchaeology of fetuses. In The Anthropology of the Fetus: Biology, Culture and Society, edited by Sallie Han, Tracy K. Betsinger, and Amy B. Scott. Berghahn Books, New York, pp. 83–111.
Hartill, V., K. Szymanska, S. M. Sharif, G. Wheway, and C. A. Johnson. 2017. Meckel-Gruber syndrome: An update on diagnosis, clinical management, and research advances. Frontiers in Pediatrics 5:244. DOI: 10.3389/fped.2017.00244.
Hefner, J. T., B. F. Spatola, N. V. Passalacqua, and T. P. Gocha. 2016. Beyond taphonomy: Exploring craniometric variation among anatomical material. Journal of Forensic Sciences 61(6):1440–1449.
Helleiner, J., V. Caputo, P. Downe, and G. Laramée. 2001. Anthropology, feminism and childhood studies. Anthropologica 43(2):135–137.
Henderson, C. Yvette, and Francisca Alves Cardoso. 2018. Identified Skeletal Collections: The Testing Ground of Anthropology? Archaeopress Publishing Ltd, Oxford.
Hendrix, N., and V. Berghella. 2008. Non-placental causes of intrauterine growth restriction. Seminars in Perinatology 32(3):161–165. DOI: 10.10523/j.semperi.2008.02.004.
Hercus, C. E., W. N. Benson, and C. L. Carter. 1925. Endemic goitre in New Zealand, and its relation to the soil-iodine: Studies from the University of Otago, New Zealand. The Journal of Hygiene 24(3–4):321–402.3. DOI: 10.1017/s0022172400008779.
Hercus, C., and G. Bell. 1964. The Otago Medical School under the First Three Deans. E. & S. Livingstone Ltd, London.
Herring, A., S. Saunders, and G. Boyce. 1991. Bones and burial registers: Infant mortality in a 19th-century cemetery from upper Canada. Northeast Historical Archaeology 20:54–70. DOI: 10.22191/neha/vol20/iss1/6.
Hildebrandt, S. 2019. The role of history and ethics of anatomy in medical education. Anatomical Sciences Education 12(4): 425–431. DOI: 10.1002/ase.1852.
Hodge, C. J. 2013. Non-bodies of knowledge: Anatomized remains from the Holden Chapel collection, Harvard University. Journal of Social Archeology 13(1):122–149. DOI: 10.1177/1469605312465692.
Hodson, C. M., and R. Gowland. 2020. Like mother, like child: Investigating perinatal and maternal health stress in post-medieval London. In The Mother-Infant Nexus in Anthropology: Small Beginnings, Significant Outcomes, edited by Rebecca Gowland and Siân Halcrow. Springer International Publishing, Cham, pp. 39–64.
Hoppa, R. D. 2000. Population variation in osteological aging criteria: An example from the pubic symphysis. American Journal of Physical Anthropology 111(2):185–191. DOI: 10.1002/(SICI)1096-8644(200002)111:2<185::AID-AJPA5>3.0.CO;2-4.
Hospitals and Charitable Institutions Act. 1885. http://www.nzlii.org/nz/legis/hist_act/hacia188549v1885n46470/. Accessed 10 December 2021.
Human Tissue Act. 2008. https://www.legislation.govt.nz/act/public/2008/0028/latest/DLM1152940.html. Accessed 10 December 2021.
Ion, A. 2021. Anatomy collections as “modern ruins”: The nostalgia of lonely specimens. Science in Context 34(2):265–279. DOI: 10.1017/S0269889722000138.
Iversen, J. K., B. H. Kahrs, E. A. Torkildsen, and T. M. Eggebø. 2020. Fetal molding examined with transperineal ultrasound and associations with position and delivery mode. American Journal of Obstetrics and Gynecology 223(6):909.e1–909.e8. DOI: 10.1016/j.ajog.2020.06.042.
Jacob, J., L. W. Nikora, and J. Ritchie. 2011. Māori children and death: Views from parents. https://hdl.handle.net/10289/5941. Accessed 10 January 2023.
Jalland, P. 1996. Death in the Victorian Family. Oxford University Press, Oxford.
Jardine, R. 1904. Clinical notes of a series of twenty-two cases of obstructed labours, including eight cases of induction of labour, four cases of symphysiotomy, and ten cases of caesarean section. Transactions of the Edinburgh Obstetrical Society 29:134–157.
Jones, D. Gareth, and S. Fennell. 1991. Bequests, cadavers and dissections: Sketches from New Zealand history. New Zealand Medical Journal 104:210–212.
Jones, D. G. 20112. The Anatomy Museum and mental illness: The centrality of informed consent. In Exhibiting Madness in Museums: Remembering Psychiatry through Collections and Display, edited by Catherine Colborne and Dolly McKinnon. Routledge, New York, pp. 161–177.
Jones, D. G., and M. I. Whitaker. 2012. Anatomy’s use of unclaimed bodies. Clinical Anatomy 25(2):246–254. DOI: 10.1002/ca.21223.
Jones, K. L., M. C. Jones, and M. Del Campo, eds. 2022. Smith’s Recognizable Patterns of Human Malformation. 8th ed. Elsevier, Amsterdam. DOI: 10.1002/9781119432692.
Kemp, W. L. 2016. Postmortem change and its effect on evaluation of fractures. Academic Forensic Pathology 6(1):28–44. DOI: 10.23907/2016.004.
Kendall, N., and H. Woloshin. 1952. Cephalhematoma associated with fracture of the skull. The Journal of Pediatrics 41(2):125–132. DOI: 10.1016/S0022-3476(52)80047-2.
Kjaer, I., J. W. Keeling, and B. Fischer Hansen. 1997. Patterns of malformations in the axial skeleton in human trisomy 13 fetuses. American Journal of Medical Genetics 70(4):421–426. DOI: 10.1002/(sici)1096-8628(19970627)70:4<421::aid-ajmg17> 3.0.co;2-j.
Knight, F. 2018. Cremation and Christianity: English Anglican and Roman Catholic attitudes to cremation since 1885. Mortality 23(4):301–319. DOI: 10.1080/13576275.2017.1382460.
Kosenko, O., C. Steinicke, H. Kielstein, and F. Steger. 2022. Fetal development in anatomical preparations of Ruysch and the Meckels in comparison. International Journal of Environmental Research and Public Health 19(22):14896. DOI: 10.3390/ijerph192214896.
Lans, A. M. 2020. Embodied discrimination and “mutilated historicity”: Archiving Black women’s bodies in the Huntington Collection. In The Bioarchaeology of Structural Violence, edited by L. A. Tremblay and S. Reedy. Springer, Cham, pp. 31–52. DOI: 10.1007/978-3-030-46440-0_3/COVER.
Lane, J. M. 2018. A Marker to Remember: Transformations in Plot Attributes from 1870s-1930s in Dunedin’s Historic Northern Cemetery. Masters’ thesis, University of Otago, Dunedin.
Lans, A. M. 2021. Decolonize this collection. Feminist Anthropology 2(1):130–142. DOI: 10.1002/fea2.12027.
Larsen, C. S. 2015. Bioarchaeology: Interpreting Behavior from the Human Skeleton. Cambridge University Press, Cambridge.
Lassi, Z. S., A. Majeed, S. Rashid, M. Y. Yakoob, and Z. A. Bhutta. 2013. The interconnections between maternal and newborn health-evidence and implications for policy. Journal of Maternal-Fetal and Neonatal Medicine 26(Suppl. 1):3–53. DOI: 10.3109/14767058.2013.784737.
Lewis, M. E. 2007. The Bioarchaeology of Children: Perspectives from Biological and Forensic Anthropology. Cambridge University Press, Cambridge.
Lewis, M. E. 2017. Paleopathology of Children. Academic Press, London.
Lewis, M. E. 2019. Skeletal dysplasias and related conditions. In Ortner’s Identification of Pathological Conditions in Human Skeletal Remains, edited by J. E. Buikstra. 3rd ed. Academic Press, London.
Liu, C., Y. Cui, J. Luan, X. Zhou, and J. Han. 2013. The molecular and cellular basis of Apert syndrome. Intractable & Rare Diseases Research 2(4):115–122. DOI: 10.5582/irdr.2013.v2.4.115.
Liversidge, H. M., and T. Molleson. 2004. Variation in crown and root formation and eruption of human deciduous teeth. American Journal of Physical Anthropology 123(2):172–180. DOI: 10.1002/ajpa.10318.
Loudon, I. 1986. Deaths in childbed from the eighteenth century to 1935. Medical History 30:1–41. DOI: 10.1017/S00257273 00045014.
Loudon, I. 1991. On maternal and infant mortality 1900-1960. Social History of Medicine 4:29–73.
Loudon, I. 2000. Maternal mortality in the past and its relevance to developing countries today. American Journal of Clinical Nutrition 72(1, Suppl.):241S–216S.
Love, J., and J. M. Wiersema. 2016. Skeletal trauma: An anthropological review. Academic Forensic Pathology 6(3):463–477. DOI: 10.23907/2016.047.
MacDonald. H. 2012. ‘A body buried is a body wasted: The spoils of human dissection.’ In The Body Divided: Human Beings and Human ‘Material’ in Modern Medical History, edited by S. Ferber and S. Wilde. Oxford University Press, Oxford, pp. 9–27.
Malik, S. 2012. Syndactyly: Phenotypes, genetics and current classification. European Journal of Human Genetics 20(8): 817–824.
Mann, R. W., K. Koel-Abt, A. Dhody, P. Mahakkanukrauh, V. J. Mann, N. Techataweewan, et al. 2021. The importance of human osteological collections: Our past, present, and future. Forensic Science International 325:110895. DOI: 10.1016/J.FORSCIINT.2021.110895.
Merwin, D. R., and E. F. Harris. 1998. Sibling similarities in the tempo of human tooth mineralization. Archives of Oral Biology 43(3):205–210. DOI: 10.1016/S0003-9969(98)00003-X.
Ministry of Health. 2015. Fetal and Infant Deaths 2013. Ministry of Health, Wellington.
Michel, J., and P. Charlier. 2011. France. In The Routledge Handbook of Archaeological Human Remains and Legislation, edited by Nicholas Márquez-Grant and Linda Fibiger. Routledge, Abingdon, pp. 151–162.
Morgan, L. M. 2002. “Properly disposed of”: A history of embryo disposal and the changing claims on fetal remains. Medical Anthropology 21(3–4):247–274. DOI: 10.1080/01459740214079.
Morgan, L. M. 2004. A social biography of Carnegie embryo no. 836. The Anatomical Record Part B: The New Anatomist 276B(1):3–7. DOI: 10.1002/AR.B.20002.
Morgan, L. 2009. Icons of Life: A Cultural History of Human Embryos. University of California Press, Berkeley.
Muller, J. L., and M. S. Butler. 2018. At the intersections of race, poverty, gender, and science: A museum mortuary for twentieth century fetuses and infants. In Bioarchaeological Analyses and Bodies, edited by P. K. Stone. Springer International Publishing, New York, pp. 71–86.
Muller, J. L., K. E. Pearlstein, and C. de la Cova. 2017. Dissection and documented skeletal collections: Embodiments of legalized inequality. In The Bioarchaeology of Dissection and Autopsy in the United States, edited by K. C. Nystrom. Springer, Cham, pp. 185–201. DOI: 10.1007/978-3-319-26836-1_9/COVER.
Munabi, I. G., S. A. Luboga, L. Luboobi, and F. Mirembe. 2016. Association between maternal pelvis height and intrapartum foetal head moulding in Ugandan mothers with spontaneous vertex deliveries. Obstetrics and Gynecology International 3815295. DOI: 10.1155/2016/3815295.
Murdoch, L. 2015. “The dead and the living”: Child death, the public mortuary movement, and the spaces of grief and selfhood in Victorian London. The Journal of the History of Childhood and Youth 8(3):378–402. DOI: 10.1353/hcy.2015.0043.
Murphy, E. M. 2011. Children’s burial grounds in Ireland (cilliní) and parental emotions toward infant death. International Journal of Historical Archaeology 15(3):409–428. DOI: 10.1007/s10761-011-0148-8.
Noe, A. 2004. The human embryo collection. In Centennial History of the Carnegie Institution of Washington: Volume V. The Department of Embryology, edited by Jane Maienschein, Marie Glitz, and Garland E. Allen. Cambridge University Press, Cambridge, pp. 21–61.
Nystrom, K. C. 2014. The bioarchaeology of structural violence and dissection in the 19th-century United States. American Anthropologist 116(4):765–779. DOI: 10.1111/AMAN.12151.
Ockwell, N. 1978. Southern Cemetery Dunedin: Burial Register Transcript. New Zealand Society of Genealogists, Dunedin.
Ockwell, N. 1982. Northern Cemetery Dunedin: Burial Register Transcript. New Zealand Society of Genealogists, Dunedin.
O’Donnell, J. M. 1991. Female Complaints: Women’s Health in Dunedin, 1885-1910. Master’s thesis, University of Otago, Dunedin. https://ourarchive.otago.ac.nz/handle/10523/8260. Accessed 16 September 2023.
Ortner, D. J. 2003. Identification of Pathological Conditions in Human Skeletal Remains. 2nd ed. Academic Press, London.
Pap, I., and G. Pálfi. 2011. Hungary. In The Routledge Handbook of Archaeological Human Remains and Legislation, edited by Nicholas Márquez-Grant and Linda Fibiger. Routledge, Abingdon, pp. 185–201.
Parkes, C. M. 1986. Bereavement: Studies of Grief in Adult Life. 2nd ed. Tavistock Publications, New York.
Pauli, R. M. 2019. Achondroplasia: A comprehensive clinical review. Orphanet Journal of Rare Diseases 14:1–4. DOI: 10.1186/s13023-018-0972-6.
Pavard, S., A. Gagnon, B. Desjardins, and E. Heyer. 2005. Mother’s death and child survival: The case of early Quebec. Journal of Biosocial Science 37(2):209–227. DOI: 10.1017/s0021932004006571.
Perinatal and Maternal Mortality Review Committee. 2018a. Methodology and Definitions for Perinatal and Maternal Mortality Review Committee (PMMRC) Reporting.Health, Quality and Safety Commission, Wellington.
Perinatal and Maternal Mortality Review Committee. 2018b. Twelfth Annual Report of the Perinatal and Maternal Mortality Review Committee.Health, Quality and Safety Commission, Wellington.
Perkins, J. M., S. V. Subramanian, G. D. Smith, and E. Özaltin. 2016. Adult height, nutrition, and population health. Nutrition Reviews 74(3):149–165. DOI: 10.1093/nutrit/nuv105.
Perry, J. N. 1983. The right of ecclesiastical burial. The Catholic Lawyer 28(4):315–335.
Pollock, Linda A. 1983. Forgotten Children: Parent-Child Relations from 1500-1900. Cambridge University Press, Cambridge.
Pool, D. Ian. 1973. Estimates of New Zealand Maori vital rates from the mid-nineteenth century to World War I. Population Studies: A Journal of Demography 27(1):117–125. DOI: 10.1080/00324728.1973.10410318.
Pool, D. Ian, A. Dharmalingam, and J. Sceats. 2007. The New Zealand Family from 1840: A Demographic History. Auckland University Press, Auckland.
Porter, F., and C. MacDonald, eds. 1996. My Hand Will Write What My Heart Dictates: The Unsettled Lives of Women in Nineteenth-Century New Zealand as Revealed to Sisters, Family and Friends. Auckland University Press, Auckland.
Ranger, A., N. Chaudhary, and D. Matic. 2010. Craniosynostosis involving the squamous temporal sutures: A rare and possibly underreported etiology for cranial vault asymmetry. The Journal of Craniofacial Surgery 21(5):1547–1550. DOI: 10.1097/SCS.0b013e3181ebe62f.
Rastogi, M. V., and S. H. LaFranchi. 2010. Congenital hypothyroidism. Orphanet Journal of Rare Diseases 5(1):17. DOI: 10.1186/1750-1172-5-17.
Richardson, R. 1987. Death, Dissection and the Destitute. Penguin, London.
Riley, D. 1988. “Am I That Name?”: Feminism and the Category of “Women” in History. Macmillan, London.
di Rocco, F., E. Arnaud, and D. Renier. 2009. Evolution in the frequency of nonsyndromic craniosynostosis: Clinical article. Journal of Neurosurgery: Pediatrics 4(1):21–25. DOI: 10.3171/2009.3.PEDS08355.
Rooks, V. J., J. P. Eaton, L. Ruess, G. W. Petermann, J. Keck-Wherley, and R. C. Pedersen. 2008. Prevalence and evolution of intracranial hemorrhage in asymptomatic term infants. American Journal of Neuroradiology 29(6):1082–1089. DOI: 10.3174/ajnr.A1004.
Rylko-Bauer, B., and P. Farmer. 2016. Structural violence, poverty and social suffering. In The Oxford Handbook of the Social Science of Poverty, edited by David Brady and Linda Burton. Oxford University Press, Oxford, pp. 47–74.
Sadetskaya, E. 2015. Infant mortality decline and its socioeconomic correlates in New Zealand. Australian Economic History Review 55(2):139–162.
Sadetskaya, E., and L. Oxley. 2012. An investigation of regional infant mortality trends in New Zealand, 1873-1940. Paper presented at the New Zealand Association of Economists Conference,Palmerston North.
Salonen, R., and R. Herva. 1990. Hydrolethalus syndrome. Journal of Medical Genetics 27(12):756–759. DOI: 10.1136/jmg.27.12.756
Sappol, M. 2002. A Traffic of Dead Bodies: Anatomy and Embodied Social Identity in Nineteenth-Century America. Princeton University Press, Princeton, NJ.
Schafer, C. 2007. Dead serious? Funeral directing in New Zealand. Sites: A Journal of Social Anthropology and Cultural Studies 4(1):95–121.
Sharma, D., S. Shastri, and P. Sharma. 2016. Intrauterine growth restriction: Antenatal and postnatal aspects. Clinical Medicine Insights: Pediatrics 10:CMPed.S40070. DOI: 10.4137/cmped.s40070.
Sheehan, J. 1878. Census of the Māori population (papers relating to the). Appendix to the Journal of the House of Representatives. https://paperspast.natlib.govt.nz/parliamentary/AJHR1878-I.2.2.2.3. Accessed 11 January 2023.
Sheikh, S., I. Ganesaratnam and H. Jan. 2013. The birth of forceps. JRSM Short Reports 4(7):1–4. DOI: 10.1177/20425333 13478412.
Shirley, M. K., T. J. Cole, O. J. Arthurs, C. A. Clark, and J. C. K. Wells. 2020. Developmental origins of variability in pelvic dimensions: Evidence from nulliparous South Asian women in the United Kingdom. American Journal of Human Biology 32:c23340. DOI: 10.1002/ajhb.23340.
Sorbe, B., and S. Dahlgren. 1983. Some important factors in the molding of the fetal head during vaginal delivery—A photographic study. International Journal of Gynecology and Obstetrics 21(3):205–212. DOI: 10.1016/0020-7292(83)90081-4.
Squires, K., and D. Piombino-Mascali. 2022. Ethical considerations associated with the display and analysis of juvenile mummies from the Capuchin catacombs of Palermo, Sicily. Public Archaeology 20(1–4):66–84. DOI: 10.1080/14655187.2021.2024742.
Statistics New Zealand. 2006. A History of Survival in New Zealand: Cohort Life Tables 1876-2004. https://statsnz.contentdm.oclc.org/digital/collection/p20045coll1/id/2853/. Accessed 11 January 2023.
Stewart, K. S., and R. H. Philpott. 1980. Fetal response to cephalopelvic disproportion. BJOG: An International Journal of Obstetrics and Gynaecology 87(8):641–649. DOI: 10.1111/j.1471-0528.1980.tb04595.x.
Stone, L. 1977. The Family, Sex and Marriage in England 1500-1800. Weidenfeld and Nicholson, London.
Sudron, E. 2021. Infants in the Anatomy Museum. Unpublished report.
Tartaglia, M., C. di Rocco, E. Lajeunie, S. Valeri, F. Velardi, and P. A. Battaglia. 1997. Jackson-Weiss syndrome: Identification of two novel FGFR2 missense mutations shared with Crouzon and Pfeiffer craniosynostotic disorders. Human Genetics 101(1):47–50. DOI: 10.1007/s004390050584.
Teather, J. L. 1990. The museum keepers: The museums association and the growth of museum professionalism. Museum Management and Curatorship 9(1):25–41. DOI: 10.1016/0260-4779(90)90023-7.
The Infanticide Case: Verdict of wilful murder. 1904. Greymouth Evening Star. https://paperspast.natlib.govt.nz/newspapers/GEST19040618.2.29. Accessed 27 May 2023.
Thesleff, Irma. 2000. Genetic basis of tooth development and dental defects. Acta Odontologica Scandinavica 58(5):191–194. DOI: 10.1080/000163500750051728.
Trapeznik, Alex. 2011. On the waterfront: The historic waterfront precinct, Dunedin, New Zealand. Public History Review 18: 65–82.
Twice a Father: Increasing the Illegitimate Birth Rate. 1908. NZ Truth, May 23. https://paperspast.natlib.govt.nz/newspapers/NZTR19080523.2.26.4. Accessed 10 December 2021.
Ubelaker, D. H. 1991. Perimortem and postmortem modification of human bone: Lessons from Forensic Anthropology. Anthropologie 29(3):171–174.
University of Otago Register of Anatomical Material (1876–1941). Department of Anatomy Records (83-115-03). Hocken Collections, Dunedin.
van Vliet, G., B. Larroque, L. Bubuteishvili, K. Supernant, and J. Legér. 2003. Sex-specific impact of congenital hypothyroidism due to thyroid dysgenesis on skeletal maturation in term newborns. The Journal of Clinical Endocrinology & Metabolism 88(5):2009–2013. DOI:10.1210/jc.2002-021735.
Vertinksy, A. T., and P. D. Barnes. 2007. Macrocephaly, increased intracranial pressure, and hydrocephalus in the infant and young child. Topics in Magnetic Resonance Imaging 18:35–51. DOI: 10.1097/RMR.0b013e3180d0a753.
Waldegrave, F. 1901. Census of the Māori population (papers relating to). Appendix to the Journal of the House of Representatives. https://paperspast.natlib.govt.nz/parliamentary/AJHR1901-I.2.4.2.43. Accessed 11 January 2023.
Ward, J. G. 1905. Public health statement by the minister of public health, the Hon. Sir J.G. Ward, K.C.M.G. Appendix to the Journal of the House of Representatives. https://paperspast.natlib.govt.nz/parliamentary/AJHR1905-I.2.4.2.53. Accessed 11 January 2023.
Watkins, R. J. 2018. The fate of anatomical collections in the US: Bioanthropological investigations of structural violence. In Identified Skeletal Collections: The Testing Ground of Anthropology? edited by Francisca Alves Cardoso and Charlotte Yvette Henderson. Archaeopress, Oxford, pp. 169–185. DOI: 10.2307/J.CTV1PDRQCT.11.
Weidig, I., C. Bis-Worch, N. Rehbach, U. Nothwang, A. Sindermann, J. Krier, et al. 2011. Luxembourg. In The Routledge Handbook of Archaeological Human Remains and Legislation, edited by Nicholas Márquez-Grant and Linda Fibiger. Routledge, Abingdon, pp. 257–265.
White, T. D., and P. A. Folkens. 2005. The Human Bone Manual. Academic Press, Burlington, MA.
Wilkie, L. A. 2003. The Archaeology of Mothering: An African-American Midwife’s Tale. Routledge, New York.
Wilson, E. K. 2015. The collection and exhibition of a fetal and child skeletal series. Museum Anthropology 38(1):15–27. DOI: 10.1111/MUAN.12070.
Zuckerman, M. K., R. M. Austin, and C. A. Hofman. 2021. Historical anatomical collections of human remains: Exploring their reinterpretation as representations of racial violence. The ANNALS of the American Academy of Political and Social Science 694(1):39–47. DOI: 10.1177/00027162211008815.
Supplementary File 1
Images of the records of Hugh Gourley (undertaker)

Figure S1. Example of Index of Gourley’s 1925–1927 ledger. Name has been redacted.

Figure S2. Example of page of transactions with the University from Gourley’s 1908–1910 ledger. Names have been redacted.
Supplementary File 2
Details of Postmortem Modifications, Pathological Descriptions, Images, and Differential Diagnoses
Postmortem Modifications
Pathological Descriptions
Individual O3.D15
An articulated crania of an individual with an estimated age of 38 to 40 weeks gestation (accession identification O3.D15) had an 11-mm overlap of the parietal bones at the sagittal suture (Supplementary Figure 5). Overlap of the parietal and occipital bones at the lambdoid suture was also visible, but the amount of overlap was unable to be measured due to the articulation of the cranial bones (Supplementary Figure 6). This overlap was likely the result of head molding during delivery. If an infant is in the correct position for delivery (head down), a large amount of pressure is distributed across the cranial vault as the fetus passes through the pelvis (Chasler 1967; Sorbe and Dahlgren 1983). The flexible cranial sutures and open fontanelles of the fetal skull allow the bones of the cranial vault to shift and overlap as the fetus moves through the pelvis during delivery (molding) and reduces the circumference of the skull, allowing for an easier passage through the birth canal (Ami 2019; Chasler 1967; Sorbe and Dahlgren 1983). Trauma to the brain from head molding can occur even in a “normal” delivery with no visible head molding from the birth process (Ami et al. 2019; Rooks et al. 2008). Severe cases of head molding can lead to intrapartum or neonatal death (Sorbe and Dahlgren 1983). Significant head molding during delivery may indicate cephalopelvic disproportion, when the size of the head of the infant and the size of the pelvic outlet are incompatible for birth (Buchmann and Libhaber 2008; Iversen et al. 2020; Munabi et al. 2016; Stewart and Philpott 1980). Without treatment, cephalopelvic disproportion may result in an obstructed labor and could be a death sentence for both the mother and child (Dolea and AbouZahr 2000; Shirley et al. 2020). Treatments such as symphysiotomy and craniotomy were available but either required long convalescence postprocedure or resulted in the death of the infant (Jardine 1904). Caesarean sections were not commonly performed in nineteenth-century New Zealand (Clarke 2012), and so an obstructed labor may have meant death or life-changing disability for both mother and child (Drife 2002; Jardine 1904). It is possible that cephalopelvic disproportion and the resulting obstructed labor was the cause of the molding observed in individual O3.D15 and may have been the primary trauma resulting in their death.
Individual O3.D6
Another individual (O3.D6) with an estimated age of 40 weeks has perimortem trauma to the right parietal bone (Supplementary Figure 7). The trauma site measures 40.4 mm from anterior to posterior and lies immediately superior to the right parietal eminence. This bone fracture displays a stellate pattern, with multiple fractures radiating from a middle area of wastage 22.3 mm in width (anterior to posterior). There is some plastic deformation of the remaining bone around this area of wastage and one fracture extending to but not crossing the coronal suture anteriorly to the trauma. Superiorly, there is another smaller area of wastage (11.6 mm from anterior to posterior). The plastic deformation of bone around an area of fracture indicates that the trauma occurred before the organic collagen component of the bone had degraded and so could have occurred around the time of death (Kemp 2016; Ubelaker 1991). Plastic deformation is the permanent bending of bonds between atoms in bone, caused by slow loading stress (Love and Wiersema 2016). A lack of remodeling or new bone growth around the fracture also supports the argument that this is perimortem trauma. Given this infant’s age and the nature of the blunt-force trauma, one possible cause of this trauma is from the use of forceps during delivery (Chasler 1967; Dupuis et al. 2005; Kendall and Woloshin 1952). Instrumental forceps deliveries were common at the time for both prophylaxis and intervention in obstructed labor (DeLee 1920).
Individual O3.D7
This individual is represented by an articulated crania with an estimated age-at-death of younger than one month post-birth. Age estimation from the dentition and the cranial size were consistent. This individual is well preserved except for postmortem damage to the maxilla and mandible, exposing the dentition. Individual O3.D7 exhibits bilateral fusion of the coronal and squamous sutures (Supplementary Figure 4). The coronal suture had also begun to obliterate. Fusion of these cranial sutures normally begins in adulthood (Cunningham et al. 2016).
Individual O3.D14
Individual O3.D14 is represented by an articulated crania with an estimated age-at-death of one to three months post-birth. Estimations of age from the dentition and the cranial bone size were consistent. Individual O3.D14 exhibits significant postmortem damage to the left and right parietal bones, exposing the dura mater that has been preserved inside the cranium. This damage has likely occurred to the thin bones during the use of the individual in medical and anatomical education at the University of Otago. This individual has evidence for developmental pathology in the form of bilateral fusion of the squamous and coronal sutures without total obliteration and abnormal frontal bossing (Supplementary Figure 8). In addition, approximately midway down, and either side of the metopic suture, there is an area of irregularity. At this level, on the right frontal bone, there is a small area of exposed dura; to the left in the same location appears to be an area of thinning bone (Supplementary Figure 9).
Individual O3.D180
The third individual represented by an articulated skull displaying pathology, individual O3.D180, was 38 to 40 weeks gestation with evidence for developmental abnormalities. This individual has an abnormally large anterior fontanelle (Supplementary Figure 10), one large intrasutural bone in the medial part of the lambdoid suture (Supplementary Figure 11), an underdeveloped face, and many very small intrasutural bones (Supplementary Figures 11 and 12).
Individual O5.D1
Individual O5.D1 is an articulated full skeleton. Age estimation from the dentition was not possible due to the remains being encased but is likely a neonate based on the individual’s size. Analysis found the frontal bone sits significantly inferior (~1 cm) to the parietals at the level of the anterior fontanelle, and the occipital contained three extra bone ossicles (intrasutural bones) in the superior portion around the level of lambda extending right and inferiorly (Supplementary Figure 13). As well as this, the anterior fontanelle appeared unusually large. Post-cranially, the axial skeleton exhibited an anteriorly protruding sternum and ribcage. The pelvis is narrow and internally rotated on the left with the developing sacrum and coccyx curving around through and above the pelvis inlet. On the appendicular skeleton, the humerus is angled medially bilaterally, creating a high carrying angle at the elbow, and there is a left deviation of both femora in the acetabulum. There is bilateral medial deviation of the feet from the metatarsals to phalanges. The left first metatarsal sits slightly under the second metatarsal. The right foot exhibited postaxial polydactyly type A (Benjamin et al. 2022) with a broad fifth metatarsal bone and no shaft duplication, but with duplication at the phalangeal level, creating six phalanges.
Differential Diagnosis
Individuals O3.D7 and O3.D14
Premature fusion of the cranial sutures or craniosynostosis is a relatively common developmental anomaly, affecting around 1/2,500 children (Aleck 2004; di Rocco et al. 2009). Untreated craniosynostosis can lead to abnormal growth of the cranium and increased intracranial pressure (Governale 2015). Most cases of craniosynostosis are isolated and are not usually inherited. These cases are known as primary nonsyndromic craniosynostosis and typically affect one cranial suture only, most commonly the sagittal suture (Aleck 2004; Governale 2015; Ranger et al. 2010). Due to the number of sutures involved in the cases of craniosynostosis in individuals O3.D7 and O3.D14, primary nonsyndromic craniosynostosis is an unlikely diagnosis (Aleck 2004; Governale 2015).
Syndromic craniosynostosis results from genetic mutations, most commonly in the fibroblast growth factor receptor (FGFR) genes (Aleck 2004; Governale 2015). Although syndromic genes can mutate spontaneously, most cases of syndromic craniosynostosis have a familial component (Governale 2015). The most common conditions that cause syndromic craniosynostosis are Crouzon syndrome, Jackson–Weiss syndrome, Apert syndrome, and Pfeiffer syndrome (Aufderheide and Rodríguez-Martin 1998). All these conditions present with craniosynostosis, along with variable cranial and midface deformities, and usually with specific diagnostic features in the post-cranial skeleton. As O3.D7 and O3.D14 are only represented by skulls, any post-cranial skeletal pathology is unable to be assessed, leaving the diagnosis inconclusive for these two individuals (Supplementary Tables 2 and 3, respectively).
Individual O3.D180
The differential diagnosis for this individual focused on conditions that result in abnormally large fontanelles and an underdeveloped face, as well as disorders of bone development and ossification, including achondroplasia, increased intracranial pressure, rickets, congenital hypothyroidism, Down syndrome (trisomy 21), Edwards syndrome (trisomy 18), and intrauterine growth restriction (Supplementary Table 4). As with the previous individuals discussed, the absence of post-cranial remains means a more conclusive diagnosis of congenital disorders is not possible. The congenital conditions consistent with most of the pathology present of this individual are Edwards syndrome (trisomy 18) or congenital hypothyroidism. Edwards syndrome is a rare genetic condition caused by the presence of one extra partial or full chromosome 18 and occurs in approximately 1 in 8,000 live births (Cereda and Carey 2012). Individuals with trisomy 18 have low birth weight, growth restriction, an underdeveloped face, a wide anterior fontanelle, and a narrow forehead with a “strawberry-shaped” skull that is brachiocephalic with a flattened occipital bone and pointed frontal bones, all consistent with O3.D180’s morphology (Supplementary Figure 10). Edwards syndrome is associated with a very high fetal and infant mortality rate, where almost 40% of affected individuals who make it to term die during labor (Cereda and Carey 2012).
Congenital hypothyroidism (CH) occurs when there is a lack of the hormones triiodothyronine and thyroxine, which stimulate metabolism and are important in the formation and maturation of bone (Rastogi and LaFranchi 2010). Congenital hypothyroidism can be permanent or transient. Permanent CH is the result of thyroid abnormalities or errors of thyroid hormone biosynthesis, while transient CH can occur due to thyroid-stimulating hormone deficiency or congenital hypopituitarism. Maternal iodine deficiency can also cause transient CH (Rastogi and LaFranchi 2010), which is important within the New Zealand context as the soil is naturally low in iodine, and goiter was common in the population prior to the introduction of iodized salt in the 1920s (Hercus et al. 1925). Signs of CH typically arise in the soft tissue, but CH can also cause abnormal development in skeletal tissue, resulting in wide anterior and posterior fontanelles, open sutures, and epiphyseal dysgenesis (Rastogi and LaFranchi 2010; van Vliet et al. 2003).
There is a discrepancy of estimated skeletal age of this individual (34–36 weeks gestation) compared with a dental age estimation of 38 to 40 weeks gestation. It is possible that this individual suffered intrauterine growth restriction as the result of a genetic condition or concurrently with a genetic condition as a result of maternal health and placental conditions (Hendrix and Berghella 2008; Sharma et al. 2016).
Individual O5.D1
When considering individual O5.D1, there are clear developmental anomalies, and diagnoses considered focused on the postaxial polydactyly, including trisomies 13 and 18, Ellis–van Creveld syndrome, and Greig cephalopolysyndactyly syndrome. While no diagnosis was definitive, O5.D1 has features suggestive of trisomy 13 (also known as Patau syndrome), chondroectodermal dysplasia (Ellis–van Creveld syndrome), and hydrolethalus syndrome (Supplementary Table 5).
Trisomy 13 presents as a multiple congenital anomaly pattern and occurs in approximately 1 in 10,000 live births (Carey 2022). First described in 1960, trisomy 13 is caused by the translocation of all or part of chromosome 13, resulting in an individual with 47 chromosomes. The cardinal signs of trisomy 13 are orofacial clefts, microphthalmia/anophthalmia, and postaxial polydactyly of the hands and feet, but these features only have 60% to 70% occurrence in the syndrome, making diagnosis challenging (Carey 2022). Soft tissue defects and organ malformations can add weight to the diagnosis, but obviously not in skeletal material such as O5.D1. The lethality of trisomy 13 depends on the degree of malformation and can vary between individuals.
Chondroectodermal dysplasia, also known as Ellis–van Creveld syndrome, was first reported in 1940, with more than 200 cases now identified. O5.D1 shares some features with chondroectodermal dysplasia, such as polydactyly of the feet, short middle phalanges, and abnormal rib development (Jones et al. 2021), but once again, diagnosis is limited as clinical diagnoses make use of abnormalities in the soft tissue. Approximately half of children born with chondroectodermal dysplasia die in early infancy, usually as a result of cardiorespiratory malformations (Jones et al. 2021).
Two disorders of primary cilium structure were also considered: Meckel–Gruber and hydrolethalus syndrome. Both syndromes are the result of genetic mutations in the genes encoding the primary cilium, and a common feature is postaxial polydactyly (Carey 2022; Hartill et al. 2017; Salonen and Herva 1990). Meckel–Gruber and hydrolethalus are considered lethal, with most infants with the disorders stillborn or dying within a few days of birth (Carey 2022; Hartill et al. 2017; Salonen and Herva 1990). Meckel–Gruber and hydrolethalus syndromes primarily manifest in the organs, with some skeletal features present.

Figure S3. View of the left side of the skull of individual O3.D6. The cranial vault has been opened using a postmortem transverse cut. (A) Arrow indicating an example of the postmortem shallow demarcation kerf mark on the left lateral frontal bone. (B) Arrow indicating the kerf marks crossing the left squamosal suture.

Figure S4. View of the left side of the skull of individual O3.D7 showing fusion and partial obliteration of the coronal and squamous sutures. Arrow indicating an example of the shallow demarcation kerf marks on the left parietal bone.

Figure S5. The overlap of the left parietal bone over the right parietal bone at the sagittal suture in individual O3.D15.

Figure S6. The overlap of the parietal bones over the occipital bone at the lambdoid suture in individual O3.D15.

Figure S7. Trauma to the right parietal bone of individual O3.D6.

Figure S8. View of the right side of the cranium of individual O3.D14 showing fusion of the squamous suture and frontal bossing. Bone fracturing is postmortem.

Figure S9. Anterior view of individual O3.D14 showing abnormal parietal bossing due to the premature fusion of the squamous and coronal sutures. Arrow indicating the area of irregularity in the region of the metopic suture.

Figure S10. The extremely wide anterior fontanelle of O3.D180.

Figure S11. The lambdoid suture of individual O3.D180, with one large and many small intrasutural bones.

Figure S12. The left side of the cranium of individual O3.D180, showing the open lambdoid, sphenoparietal and occipitomastoid sutures, and intrasutural bones. The small midface is also visible.

Figure S13. Posterior view of the cranium of individual O5.D1, showing the three wormian bones at the level of lambda.

Figure S14. Left lateral view of individual O5.D1, showing the frontal bone sitting inferiorly to the parietal bone, as well as the abnormally protruding ribs and sternum.

Figure S15. Posterior view of individual O5.D1, showing the high carrying angles in the upper limb, internal rotation of the pelvis, and left deviation of the femur.

Figure S16. The feet of individual O5.D1, with post-axial polydactyly type A (Benjamin et al. 2022) of the right foot.
Supplementary Table S1. Death information for the babies listed in the University of Otago Register for Anatomical Material, supplemented with information from official death certificates.
|
Age at Death |
Year |
Official Death Certificate |
Father Recorded |
Father Occupation |
Place of Death* |
Cause of Death (Death Certificate) |
Cause of Death (Register of Human Material) |
Record of Burial |
|
3 days |
1885 |
No |
— |
— |
Hospital (Register) |
— |
— |
Not found |
|
15 days |
1903 |
Yes |
Recorded |
Groom |
Nelson St, South Dunedin (Dunedin Hospital) |
Malformation, inanition |
Heart |
Not found |
|
6 hours |
1913 |
Yes |
Not recorded |
— |
Maternity Hospital Forth Street (later renamed Batchelor Hospital) |
Prematurity |
Premature |
Not found |
|
6 days |
1915 |
No |
Recorded |
— |
Hospital (Register) |
— |
Spina bifida |
Not found (found birth certificate, not death certificate) |
|
14 days |
1916 |
Yes |
Not recorded |
— |
Salvation Army Home, Dunblane St, Roslyn ("Redroofs") |
Congenital heart disease |
— |
Not found |
|
3 days |
1916 |
No |
— |
— |
Dunedin Hospital (Register) |
— |
Syphilis |
Not found |
|
10 hours |
1917 |
Yes |
Not recorded |
— |
Salvation Army Home, Dunblane St, Roslyn ("Redroofs") |
Cerebral compression during delivery |
Cerebral hemorrhage |
Not found |
|
6 weeks |
1918 |
No |
— |
— |
"Redroofs" (Register) |
— |
TB enteritis |
Not found |
|
1.5 hours |
1919 |
No |
— |
— |
Dunedin Hospital (Register) |
— |
Prematurity |
Not found |
|
5 weeks |
1920 |
Yes |
Not recorded |
— |
Dunedin Hospital |
Pyloric stenosis |
Pyloric stenosis malnutrition |
Not found |
|
2 days |
1921 |
Yes |
Recorded |
Bricklayer |
Batchelor Hospital |
Congenital defect in heart |
Congenital defect in heart |
Not found |
|
2 days |
1921 |
Yes |
Not recorded |
Maternity Hospital Forth St (Batchelor Hospital) |
Immaturity |
Prematurity |
Not found |
|
|
2 days |
1925 |
Yes |
Recorded |
Carpenter |
Batchelor Hospital |
Immaturity |
Prematurity |
Not found |
|
1 days |
1926 |
Yes |
Recorded |
— |
Batchelor Hospital |
Tracheal obstruction |
Large thyroid gland, tracheal obstruction |
Not found |
|
20 minutes |
1926 |
No |
— |
— |
— |
— |
Prematurity |
Not found |
|
6 days |
1926 |
Yes |
Recorded |
Clerk |
Batchelor Hospital |
Hemorrhage neonatorum |
Hemorrhage |
Not found |
|
32 hours |
1928 |
Yes |
Recorded |
Blacksmith |
Batchelor Hospital |
Anencephalous |
Malformation |
Not found |
|
2 days |
1928 |
Yes |
Recorded |
Driver |
Batchelor Hospital |
Immaturity |
Prematurity (?), debility, etc. |
Not found |
|
2 day |
1929 |
Yes |
Not recorded |
— |
Batchelor Hospital |
Prematurity |
Prematurity, debility, cardiac condition |
Not found |
|
28 hours |
1930 |
Yes |
Recorded |
Laborer |
Batchelor Hospital |
Immaturity |
Immaturity |
Not found |
|
6 day |
1931 |
Yes |
Not recorded |
— |
Public Hospital Dunedin |
Inanition |
Inanition |
Not found |
|
4 hours |
1934 |
Yes |
Recorded |
Laborer |
Batchelor Hospital |
Neonatal asphyxia |
Congenital defects |
Not found |
|
6 hours |
1934 |
Yes |
Recorded |
Laborer |
Maternity Home, Gisborne |
Imperfect development monster |
Imperfect development. Anencephaly. Monster |
— |
|
9 days |
1936 |
No |
— |
— |
Dunedin Hospital (Register) |
— |
Inanition |
Not found |
*Register in parentheses is denoted if there was no information on the death certificate and information was obtained from the University of Otago Register of Human Material.
Supplementary Table S2. Features considered in the differential diagnosis for individual O3.D7.
|
Possible Diagnosis |
Skeletal Features |
Present (✔), Absent (x), or Unobservable (–) in O3.D7 |
Source |
|
Primary nonsyndromic craniosynostosis |
Single suture synostosis (normally sagittal) |
x |
Aleck 2004 |
|
Crouzon syndrome (not typically recognizable until end of the first year) |
Craniosynostosis |
✔ |
Aleck 2004 |
|
Jackson–Weiss syndrome |
Craniosynostosis |
✔ |
Tartaglia et al. 1997 |
|
Apert syndrome |
Craniosynostosis |
✔ |
Liu et al. 2013 |
|
Pfeiffer syndrome |
Craniosynostosis (coronal and sagittal) |
✔ (coronal only) x |
Giancotti et al. 2017 |
Supplementary Table S3. Features considered in the differential diagnosis for individual O3.D14.
|
Possible Diagnosis |
Skeletal Features |
Present (✔), Absent (x), or Unobservable (–) in O3.D14 |
Source |
|
Primary nonsyndromic craniosynostosis |
Single suture synostosis (normally sagittal) |
x |
Aleck 2004 |
|
Crouzon syndrome (not typically recognizable until end of the first year) |
Craniosynostosis |
✔ |
Aleck 2004 |
|
Jackson–Weiss syndrome |
Craniosynostosis |
✔ |
Tartaglia et al. 1997 |
|
Apert syndrome |
Craniosynostosis |
✔ |
Liu et al. 2013 |
|
Pfeiffer syndrome |
Craniosynostosis (coronal and sagittal) |
✔ (coronal only) x |
Giancotti et al. 2017 |
Supplementary Table S4. Features used in the differential diagnosis of individual O3.D180.
|
Possible Diagnosis |
Skeletal Features |
Present (✔), Absent (x), or Unobservable (–) in 03.D180 |
Source |
|
Achondroplasia |
Macrocephaly |
x |
Pauli 2019 |
|
Increased intracranial pressure |
Macrocephaly |
x |
Vertinsky and Barnes |
|
Rickets (features usually visible after four months of age) |
Thin bone |
x |
Brickley and Ives 2008 |
|
Congenital hypothyroidism |
Wide anterior fontanelle |
✔ |
Rastogi and LaFranchi |
|
Trisomy 21 (Down’s syndrome) |
Delayed ossification |
x |
Barden 1983 |
|
Trisomy 18 (Edwards’ syndrome) |
Prominent occiput |
✔ |
Cereda and Carey 2012 |
|
Intrauterine growth restriction (IUGR) |
Macrocephaly (not in symmetrical IUGR) |
x |
Sharma et al. 2016 |
Supplementary Table S5. Features used in the differential diagnosis of O5.D1.
|
Possible Diagnosis |
Skeletal Features |
Present (✔), Absent (x), or Unobservable (–) in O5.D1 |
Source |
|
Trisomy 13 (Patau Syndrome) |
Sloping forehead |
x |
Kjaer et al. 1997 |
|
Trisomy 18 (Edwards’ syndrome) |
Prominent occiput |
x |
Cereda and Carey 2012 |
|
Chondroectodermal dysplasia (Ellis–van Creveld syndrome) |
Small stature of prenatal onset |
– – |
Jones et al. 2021 |
|
Greig cephalopolysyndactyly syndrome |
High forehead |
x |
Jones et al. |
|
Meckel–Gruber syndrome |
Postaxial polydactyly of hands and |
✔ x x |
Hartill et al. 2017 |
|
Hydrolethalus syndrome |
Occipital bone defect |
x |
Salonen and Herva 1990 |
#These authors contributed equally to this work.
aDepartment of Anatomy, University of Otago, Dunedin, New Zealand
bAustralian Research Centre for Human Evolution, Griffith University, Gold Coast, Australia
*Correspondence to: Siân E. Halcrow, University of Otago, Anatomy, Great King Street, Dunedin 9054, New Zealand
E-mail: sian.halcrow@otago.ac.nz